Article Text

Abstract
Background Poor core stability is linked to a range of musculoskeletal pathologies and core-strengthening programmes are widely used as treatment. Treatment outcomes, however, are highly variable, which may be related to the method of delivery of core strengthening programmes. We investigated the effect of identical 8 week core strengthening programmes delivered as either supervised or home-based on measures of core stability.
Methods Participants with poor core stability were randomised into three groups: supervised (n=26), home-based (n=26) or control (n=26). Primary outcomes were the Sahrmann test and the Star Excursion Balance Test (SEBT) for dynamic core stability and three endurance tests (side-bridge, flexor and Sorensen) for static core stability. The exercise programme was devised and supervised by an exercise physiologist.
Results Analysis of covariance on the change from baseline over the 8 weeks showed that the supervised group performed significantly better on all core stability measures than both the home-based and control group. The home-based group produced significant improvements compared to the control group in all static core stability tests, but not in most of the dynamic core stability tests (Sahrmann test and two out of three directions of the SEBT).
Conclusions Our results support the use of a supervised core-strengthening programme over a home-based programme to maximise improvements in core stability, especially in its dynamic aspects. Based on our findings in healthy individuals with low core stability, further research is recommended on potential therapeutic benefits of supervised core-strengthening programmes for pathologies associated with low core stability.
Trial registration number ACTRN12613000233729.
- Core stability
- Exercise rehabilitation
- Training
- Intervention efficacy
Statistics from Altmetric.com
Introduction
Core stability refers to the ability of core musculature to stabilise the spine.1 It is required to increase stiffness of the trunk and hip in preparation for, and in response to, spinal loading, to prevent instability of the vertebral column and to facilitate return to equilibrium following perturbation.2 Poor core stability is linked to development of a range of musculoskeletal pathologies of the spine and lower extremities, including low back pain3 and over-use injuries of the hip, knee, ankle and foot.4–6
Core strengthening programmes aim to improve core stability by developing strength, endurance and neuromuscular control of core muscles.7 Such programmes are currently recommended as a primary treatment for chronic low back pain.8 Despite widespread use, treatment outcomes are highly variable and the efficacy of this exercise approach for treatment of pathology remains unclear.9 ,10
A possible source of the heterogeneity of therapeutic outcomes following core-strengthening programmes is the method of programme delivery, with both supervised and home-based programmes in common use. Home-based exercise programmes of any type offer several benefits over supervised programmes including greater flexibility for patients and reduced associated healthcare system costs. However, home-based programmes rely on the participants’ motivation and ability to correctly perform the exercises independently, and self-reported compliance is similar to, or lower than, supervised programmes.11
To date there has been little investigation of the effect of home-based versus supervised exercise programmes for core stability. Bronfort et al12 found better results with a supervised core-strengthening programme. However, as different exercises were used for the home-based and supervised group, it was not possible to determine if this was due to the delivery method or the specific exercises used. Poorer outcomes for home-based core strengthening programmes may be related to the difficulty participants have effectively performing exercises without external feedback. Specific instructions, as are given under supervision, induced improved activation of deep core stabilising muscles during trunk flexion activities.13 It is unknown, however, to what extent the absence of such instruction affects the efficacy of a home-based programme. Thus, we determined the effect of identical core-strengthening programmes delivered as either a (1) supervised or (2) home-based programme compared to (3) no intervention on measures of core stability.
Methods
This was a three-arm, stratified (gender, age) with balanced randomisation, single-blind, controlled, parallel-group study conducted on the University of Newcastle Central Coast Campus. This project was approved by the institutional Human Research Ethics Committee and was registered with the Australian and New Zealand Clinical Trials Registry (available at http://www.ANZCTR.org.au/ACTRN12613000233729.aspx). Participants were recruited on a volunteer basis from staff and students via flyer advertising.
Inclusion criteria were 18 years of age or over with a Sahrmann test score of level 1 or lower indicating poor core stability. Exclusion criteria included current pregnancy, current acute specific low back pain, current acute lower limb injury or any musculoskeletal, neurological, systemic or local pathology affecting balance, neuromuscular control or altering muscle response to exercise and current or previous participation in any form of core-strengthening programme.
Randomisation
Participants were randomised into the intervention or control groups with a software randomisation function by a researcher independent of the trial. Randomisations were stratified for age and gender.
Interventions
This trial used two interventions and a control. The first intervention was a supervised core-strengthening programme which was performed over 8 weeks, with participants required to attend two classes per week.1 ,14–20 Details of the programme and rationale for included exercises are provided in online supplementary file 1. This programme was conducted by an exercise physiologist not involved in recruitment or testing who provided instruction, demonstration and individual feedback on correct execution of exercises. Compliance at these sessions was monitored via an attendance record completed by the exercise physiologist.
The second intervention was a home-based core-strengthening programme. Participants in the home-based programme received an initial instructional class in which they were taught the principles of deep abdominal muscle activation and the progression of all exercises used in the programme. They were also provided with written and diagrammatic instructions to follow for two sessions per week for 8 weeks. All exercise sessions in the home-based programme were identical to those in the supervised programme. All instructional sessions were provided by the same exercise physiologist who ran the supervised group classes. Compliance was assessed using a self-reported compliance questionnaire.
The third group served as controls and participated in baseline and follow-up testing only. All groups were instructed not to change their physical activity levels outside the prescribed programmes.
Procedures
Potential participants were initially screened using the Sahrmann test. Participants achieving a score of level one or less were then eligible to enter the trial. The baseline testing consisted of the Sahrmann test to evaluate dynamic lumbopelvic stability,21 ,22 three tests of static trunk muscle endurance requiring sustained isometric contraction, (the side bridge endurance test,14 the flexor endurance test18 and the Sorensen test23) and the Star Excursion Balance Test (SEBT)24–26 to assess dynamic postural stability in three directions (anterior, posterolateral and posteromedial).27 Details of and rationale for these tests are provided in online supplementary file 2.
The participants were then randomised to one of the three groups. The trial began once 13 participants had been recruited for the supervised core-strengthening group to allow for adequate class size. Within 1 week of completion of the 8 week intervention all participants performed the same tests as at baseline. All assessments were performed by the same researcher, who was blinded to participant group allocation.
Test–retest reliability of all core stability tests was assessed on a separate group of 15 participants who met the main study inclusion criteria. Following baseline testing these participants returned 7–10 days later and repeated all core stability assessments. The testing was completed by the same researcher who performed baseline and follow-up testing.
A sample size of 26 per group was calculated based on a minimally important change of 7% for the SEBT assuming a SD of 10%, a power of 90%, an α of 0.05 and allowing for 10% attrition rate.28
Outcomes
Primary outcomes were change in dynamic lumbopelvic stability measured with the Sahrmann test, change in independent measures of static core stability assessed with the side bridge endurance test, the flexor endurance test and the Sorensen test and, change in dynamic postural stability measured with the SEBT. Secondary outcomes were compliance with the intervention and adverse events.
Statistical analysis
Statistical analysis was conducted on a blinded, intention-to-treat basis using SPSS software (V.21.0 SPSS Chicago, Illinois, USA). For the primary outcomes, data were analysed with analysis of covariance (ANCOVA) using a linear regression approach to investigate change from baseline following the 8 week intervention for each variable. The baseline measure was the only covariate used in each analysis. Cohen's d was used to calculate effect sizes. An effect size of greater than or equal to 0.8 was considered to represent a large clinical effect, 0.5 a moderate effect and 0.2 a small effect.29 Correlations were performed between all measures of core stability and self-reported and recorded compliance for the home-based and supervised group, respectively.
For the reliability component intraclass correlation coefficients (ICC) with 95% CI were calculated to determine level of agreement between test and retest for all measurements. All ICC values for test–retest reliability were interpreted according to criteria recommended by Fleiss.30 Paired t tests were performed to determine whether statistically significant differences existed between sessions.
Results
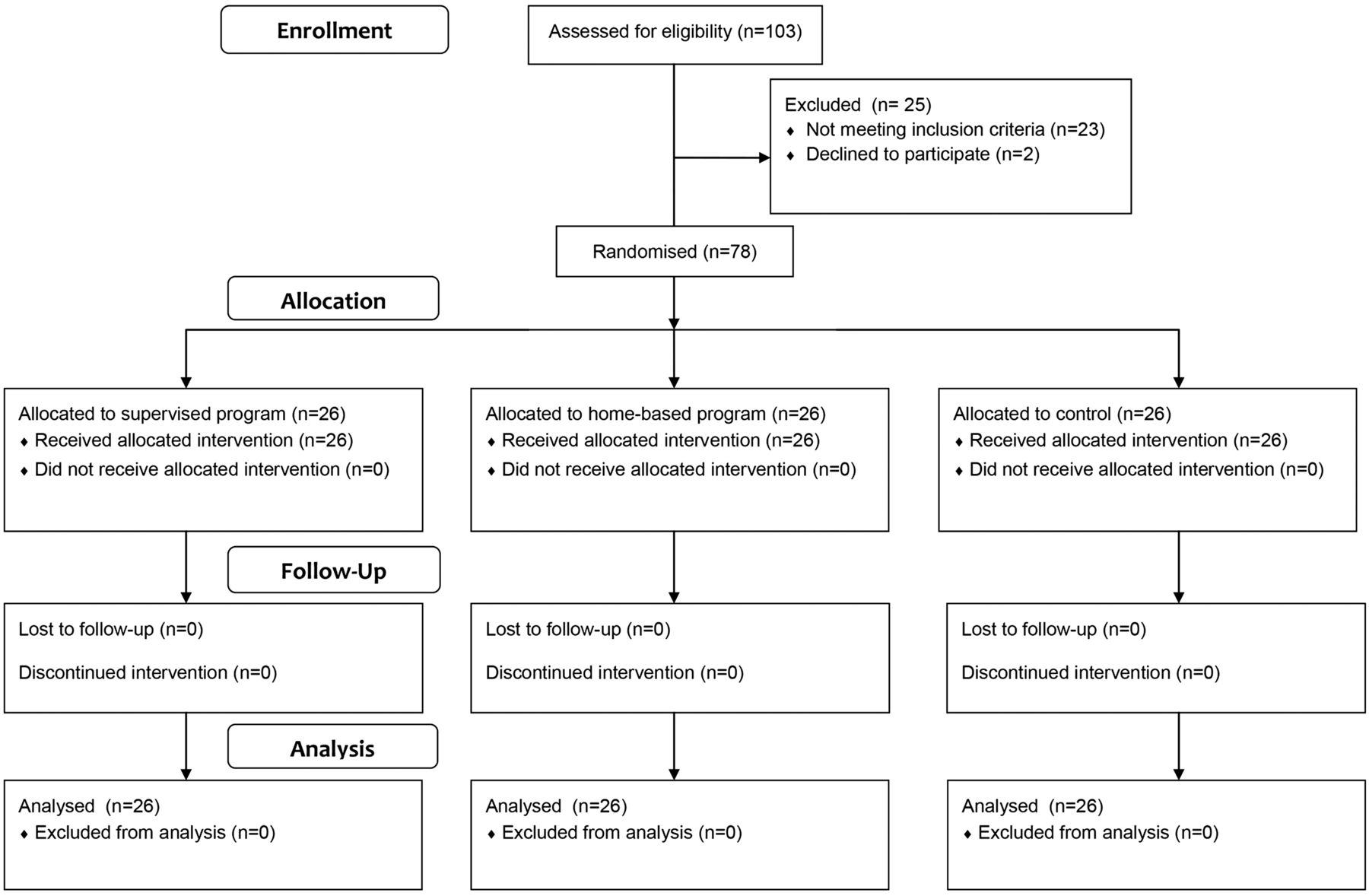
Seventy-eight participants were recruited between June and September 2012. Participant characteristics are included in table 1. Figure 1 demonstrates participants’ progression through the trial. Participants in the supervised core strengthening programme attended approximately 76% (12.1) of the 16 scheduled classes for their programme. Those in the home-based programme self-reported a higher mean compliance rate with an average of 85% (13.6) of the 16 sessions completed. The trial was ended once 26 participants had completed each intervention. The characteristics of the reliability group are also shown in table 1.
Participant characteristics
{kind=link}
CONSORT flow diagram of participants’ progression through the trial.
Measures of core stability
Participants in the supervised core-strengthening programme demonstrated more statistically significant improvements in mean scores on all measures of core stability than those in the home-based programme and the control group and effect sizes were generally moderate to large (tables 2 and 3) and significant for the Sahrmann and Sorenson tests. The home-based programme produced significant improvements compared to the control group in most tests, except for the Sahrmann test and the SEBT posterolateral and posteromedial directions which had small to moderate effect sizes (tables 2 and 3).
Adjusted means for follow-up core stability testing
Effect sizes (Cohen's d) in mean (95% CI) and p values for difference in adjusted means between groups at follow-up
Correlations
Correlations between compliance and outcomes of tests of core stability were strongest for the supervised group (table 4). Significant positive correlations were demonstrated between the number of sessions attended in the supervised group and all core stability outcomes, except for the side bridge. In the home-based programme only outcomes for the flexor endurance test were positively correlated with self-reported compliance (table 4).
Correlations between compliance and measurement outcomes at follow-up testing for the supervised and home-based groups
Reliability
Test–retest reliability for functional tests of core stability was excellent with ICCs ranging from 0.80 to 0.91 (table 5). Paired samples t tests demonstrated no significant differences between test and retest measures.
Test–retest reliability
Adverse events
There were no reported adverse events associated with this research.
Discussion
We found that a supervised core-strengthening programme results in significantly greater improvements in static and dynamic core stability measures than an identical home-based programme. The home-based programme's effect was restricted to greater static core muscle endurance compared to the control group and may have been influenced by the similarity between some of the less complex exercises and the specific tests used, for example side-bridge endurance. This finding may have therapeutic relevance as greater isometric core muscle endurance in the three static tests selected for the current study is associated with better spine stability during most activities.14
Supervised intervention provides superior outcome
In general, supervised exercise interventions are more effective than home-based interventions.11 ,31–33 Bronfort et al12 also showed greater improvement in trunk muscle endurance in people undertaking supervised classes compared to those doing a different exercise programme at home. Based on the outcomes of the current trial, it is likely that the difference in method of programme delivery used by Bronfort et al12 may largely explain the superior outcomes in the supervised group, independent of the different types of exercises being used. Our use of the same exercise programme for both the home-based and supervised groups in the present study clearly demonstrates that the delivery method of the programme has a significant influence on the outcomes of core-strengthening programmes.
For the dynamic measures of core stability the supervised programme again produced significantly better results than the home-based programme. Furthermore the home-based programme failed to produce any significant improvement in the Sahrmann test and the posterolateral and posteromedial directions of the SEBT compared to the control condition. Although there was a significant improvement in the anterior direction of the SEBT by those in the home-based programme compared to the control group, the improvement in the supervised group was significantly greater.
The Sahrmann test assesses spinal stability with and without movement of the lumbopelvic complex,16 whereas the SEBT measures dynamic stability with poorer performance associated with mechanical or sensorimotor deficits.34 Our findings suggest that a home-based unsupervised core-strengthening programme may be less effective for neuromuscular retraining and produces less improvement in core stability during dynamic tasks than a supervised programme. Previous research demonstrated improved activation of deep core stabilising muscles during trunk flexion activities in association with verbal and tactile cues.13 Instruction on stabilisation also altered the motor control strategy of trunk musculature and produced increased lumbar spine control during upper and lower body movements.35 Although participants in the home-based group in our trial received initial verbal instruction, demonstration and written instruction on performance of all exercises, our results suggest this was not sufficient to achieve significant change in neuromuscular control strategies to improve dynamic core stability. This may be related to a lack of understanding of the progression of exercises demonstrated in the initial instruction session potentially resulting in reduced compliance or participants performing more demanding tasks incorrectly.
Compliance
Self-reported compliance in the home-based programme was higher than recorded attendance for the supervised group. However, correlations between compliance and pre-test and post-test change in core stability measures demonstrated stronger associations in the supervised group. This may have been due to more effective training in the supervised programme, but may also have been influenced by over-reporting of compliance in the home-based group. Although increased attendance at the supervised classes was associated with improved performance across all tests, the strongest relationships occurred with the Sahrmann test, the posteromedial and posterolateral SEBT. These results suggest increased adherence to supervised training programmes may produce better outcomes for more demanding dynamic tasks that not only require increases in core muscle strength, but also high levels of neuromuscular control. The strong association between the compliance and both the flexor endurance and the Sorensen tests suggests maintaining the training programme as close to two sessions per week as possible can produce better trunk flexor and extensor endurance.
In the home-based programme the strength of association between self-reported compliance and change in measured outcomes was generally low. This may have been due to a smaller effect on outcome measures of the exercise programme conducted in a non-supervised environment or due to over-reporting of compliance. The significant positive correlation for flexor endurance with the number of sessions performed, in conjunction with the significant improvement seen for this outcome postintervention, suggests participants may have performed exercises targeting the anterior abdominal muscles more frequently or with better technique. High reported compliance with the intervention and small changes in measured outcomes may also have confounded other potential associations.
Outcome measure reliability
Test–retest reliability was performed for all outcome measures in this trial. This was not our primary aim and the assessments used have been demonstrated previously to have adequate reliability.3 ,21 ,35–38 However, the subjective nature of the end point of several of the tests, where the researcher was required to specify the time point at which a participant ‘failed’ based on observation, meant establishing reliability of assessments specifically for this trial was warranted. The ICCs ranging from 0.80 to 0.91 indicated excellent test–retest reliability and were consistent with existing literature.3 ,21 ,35–38 No change in values between test sessions is a further indicator of good test–retest reliability. This indicates that improvements in outcome measures for the home-based and supervised training programmes represent true changes as a result of the intervention.
Limitations
Our findings support the use of a supervised programme over a home-based programme for improving static core muscle endurance and dynamic core stability. This study targeted participants with poor dynamic core stability, with trial inclusion requiring a Sahrmann test performance of level one or less. Participants with current pathology that may be attributable to poor core stability, such as low back pain, were excluded. Therefore, although it is evident from this trial that participants with poor dynamic core stability demonstrate an improved response to core training in a supervised environment, it is not known if this translates to exercise intervention for pathologies, such as low back pain, where the initial level of dynamic core stability may be more variable. Existing evidence has demonstrated altered function of deep core stabilising muscles, such as transversus abdominis, during activity in people with low back pain.3 This suggests that improving dynamic core stability is an essential component of rehabilitation for low back pain. The current trial findings indicate that a supervised core strengthening programme may be advisable, but further investigation on specific cohorts, including those with low back pain,39 needs to be undertaken to determine if supervised programmes also provide the best results in those cohorts.
A further limitation of this study was the nature of the core strengthening programme delivered. The same programme was given to both the supervised and home-based groups to isolate the effect of method of delivery on core muscle endurance and dynamic stability. However, due to the reliance on the participant to perform the exercises in an ongoing manner following initial instruction, a home-based programme may require a different approach. Home-based programmes may benefit from including specific exercises more congruent with being performed without instruction to maximise outcomes. Investigation of effectiveness of specific types of programmes delivered in a home-based environment needs to be undertaken to develop a more effective method for core strengthening to be undertaken without supervision. In addition the outcomes of supervised programmes may be influenced by the method of instruction. While it was not the purpose of this study to investigate the role of the instructor this is also an important area for further investigation.
Conclusion
The results of this study support the use of a supervised core-strengthening programme over a home-based programme to maximise improvement in static core muscle endurance and dynamic core stability in a healthy population with low core stability. Further research is recommended to assess if a supervised core-strengthening programme will also provide a greater therapeutic benefit than a similar home-based programme for pathologies associated with reduced core stability, such as low back pain.
What are the new findings
-
Supervised core-strengthening programmes result in better static and dynamic core stability outcomes than home-based programmes.
-
Home-based core strengthening programmes improve static core endurance, but not dynamic core stability.
-
Training compliance in the supervised programme was positively correlated with most core stability outcomes.
How might it impact on clinical practice in the near future
-
Supervised core strengthening-programmes may provide greater treatment benefits for musculoskeletal pathologies associated with poor core stability than home-based programmes.
-
Home-based core-strengthening programmes may be prescribed to improve static core stability, but are not likely to improve dynamic core stability.
-
Supervised core-strengthening programmes are needed to improve core stability for more demanding dynamic tasks.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
-
Contributors VHC and XAKJdJ planned the randomised controlled trial. VHC, XAKJdJ and BMT conducted the trial. All authors contributed to the reporting of the trial.
-
Funding This research was supported by funding from the Priority Research Centre for Physical Activity and Nutrition, The University of Newcastle, Australia.
-
Competing interests None.
-
Ethics approval Human Research Ethics Committee of the University of Newcastle Australia (protocol # H-2012-0013).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The corresponding author can be contacted for access to the data presented in this manuscript.