Article Text

Abstract
Objective This systematic review and meta-analysis sought to rigorously examine mental health outcomes following paediatric concussion. To date, heterogeneous findings and methodologies have limited clinicians’ and researchers’ ability to meaningfully synthesise existing literature. In this context, there is a need to clarify mental health outcomes in a homogeneous sample, controlling for key methodological differences and applying a consistent definition of concussion across studies.
Design Systematic review and meta-analysis.
Data sources We searched Medline, Embase, PsycINFO, CINAHL, SportDiscus, Scopus and PubMed.
Eligibility Peer-reviewed studies published between 1980 and June 2020 that prospectively examined mental health outcomes after paediatric concussion, defined as per the Berlin Consensus Statement on Concussion in Sport.
Results Sixty-nine articles characterising 60 unique samples met inclusion criteria, representing 89 114 children with concussion. Forty articles (33 studies) contributed to a random effects meta-analysis of internalising (withdrawal, anxiety, depression, post-traumatic stress), externalising (conduct problems, aggression, attention, hyperactivity) and total mental health difficulties across three time points post-injury (acute, persisting and chronic). Overall, children with concussion (n=6819) experienced significantly higher levels of internalising (g=0.41–0.46), externalising (g=0.25–0.46) and overall mental health difficulties compared with controls (g=0.18–0.49; n=56 271), with effects decreasing over time.
Summary/conclusions Our review highlights that mental health is central to concussion recovery. Assessment, prevention and intervention of mental health status should be integrated into standard follow-up procedures. Further research is needed to clarify the mechanisms underlying observed relationships between mental health, post-concussion symptoms and other psychosocial factors. Results suggest that concussion may both precipitate and exacerbate mental health difficulties, thus impacting delayed recovery and psychosocial outcomes.
- concussion
- psychology
- meta-analysis
- sports medicine
- paediatrics
Statistics from Altmetric.com
Introduction
Concussion is a growing public health concern with one-third of children experiencing a head injury before age 13 years.1 Despite the incidence of concussion among children and adolescents, identifying young people at risk of ongoing difficulties after concussion remains a prominent challenge in the field.2 Further, evidence shows that children take twice as long to recover from concussion than adults, with one in four children experiencing symptoms beyond 1 month post-injury, defined here as delayed recovery.3–5 Important differences in the mechanism and context blur the differentiation of sports and non-sports concussion in children and limit the translation of adult findings to paediatric concussion.6 For example, paediatric concussions are less likely to be sports related and more likely to be due to falls sustained in play or leisure, and more likely to occur in the home or in non-competitive activities.7 Child and adolescent athletes are also distinguished from older athletes along several dimensions, including biomechanical and pathophysiological responses, and contextual demands (eg, learning vs work).8
After concussion, due to either sport or non-sport injuries, children and adolescents are susceptible to a broad range of physical, behavioural, emotional, cognitive, somatic and sleep-related symptoms,9 many of which overlap with common mental health symptoms. Indeed, evidence suggests that post-concussive symptoms (PCS) correlate highly with internalising symptoms such as anxiety10 and depression,11 12 with premorbid mental illness identified as a key risk factor for delayed recovery.13 Mental health screening may provide an avenue for early detection and targeted interventions for children at risk of delayed recovery due to mental health symptoms. Despite the potential role that these behavioural and emotional disturbances may play in delayed recovery, few studies have rigorously examined this relationship.14
Research designs employed in studies investigating mental health outcomes after paediatric concussion have, to date, been heterogeneous, limiting opportunities for qualitative and quantitative synthesis.14 Variable definitions of concussion adopted across studies are a key contributing factor to this heterogeneity. Further, combining traumatic brain injury (TBI) severity groups for analysis, unclear eligibility criteria (eg, pre-injury mental health status), differences in recruitment methods (eg, inpatient, outpatient, community), nature of comparison groups and timing of outcome measurement all contribute to variability. Not surprisingly, results are also inconsistent with some studies reporting persistent mental health symptoms,15–18 while others report no such findings.19 20
Despite methodological challenges, several robust findings are reported in the literature. Female adolescents are particularly vulnerable to internalising difficulties such as depression, anxiety and withdrawal after concussion.21 Meanwhile, externalising behaviours, such as conduct problems, attention difficulties, hyperactivity and temper problems are more common among younger children.22 Whether these findings reflect risk factors associated with participant factors, such as age and sex, versus design characteristics require further exploration.
Two previous reviews have examined psychiatric outcomes from paediatric mild TBI (mTBI), however, both merged concussion, mTBI and complicated mTBI in their syntheses.14 23 These reviews emphasise high levels of variability in study findings, concluding that evidence for mental health difficulties following paediatric mTBI is inconclusive. Nonetheless, several important distinctions between these diagnoses should be acknowledged. In mTBI, recovery profiles for injuries with and without structural brain abnormalities display distinct characteristics, with structural injuries associated with slower recovery and poorer functional outcomes across cognitive, academic and social domains than when no structural injury is detected.24–31 In the present study, we have applied the definition of concussion from the Berlin Consensus Statement of Concussion in Sport (CISG), specifically ‘an acute functional disturbance coupled with post-concussion symptoms, but without evidence of structural brain injury and generally associated with the expectation of better recovery than mTBI’.9 While this definition was derived with a focus on sports concussion, it refers to injury consequences and is equally applicable to concussions sustained outside organised sport.
The objective of this review was to systematically examine prospective mental health outcomes following paediatric concussion, applying a consistent definition of concussion across studies. Specifically, we sought to address the following research questions: (1) How common are mental health difficulties after paediatric concussion? (2) What factors predict mental health following paediatric concussion? (3) How do mental health problems interact with recovery from concussion? and (4) How does mental health status change with time post-injury? We conducted a meta-analysis to determine if children experienced elevated mental health difficulties after concussion compared with controls.
Materials and methods
Protocol registration
The review protocol was registered with the International Prospective Register of Systematic Reviews (#147741).
Methods
This systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and identified articles published from 1980 to June 2020 using the search strategy shown in online supplemental table 1. This time frame was selected due to the considerable changes in the understanding of concussion over the past 40 years and the large number of articles identified in preliminary searches. The final search was conducted in June 2020. Studies identified through systematic searches of Medline, Embase, PsycINFO, CINAHL and SportDiscus. Keyword only searches were conducted through Scopus and PubMed to identify articles not captured via the above sources. Two postgraduate authors (AG, TM) independently screened titles and abstracts using Covidence Systematic Review Software.32 Articles identified as relevant in this phase were reviewed in full text (AG, XL), according to the eligibility criteria outlined below. Reviewers were blind to one another’s decision at the time of voting. Any discrepancies highlighted by the software were resolved by consensus, and a third senior clinical researcher (MT) was consulted if additional expertise was required.
Supplemental material
Eligibility criteria
This review included peer-reviewed articles reporting prospective mental health outcomes following concussion in paediatric populations (age 0–18 years at time of injury). To increase the application of present findings to inform policy and practice, this review considered quantitative, qualitative and mixed-methods studies. Quantitative studies included observational designs, prospective and retrospective cohort studies, case–control studies and analytical cross-sectional studies. Qualitative studies included, but were not limited to, phenomenology, grounded theory, ethnography and action research. Mixed-method studies were considered if data from the quantitative or qualitative components could be extracted.
Concussion was defined according to the Berlin CISG Criteria and required diagnosis by a health professional or administration of a clinically validated measure.9 The Berlin CISG Criteria were developed using rigorous methodology, including systematic review of the literature and expert panel consensus. Studies were eligible for inclusion if the concussion definition was consistent with the Berlin CISG Criteria, regardless of whether or not these criteria were explicitly cited.
Seventeen authors were contacted to clarify whether participants satisfied present criteria for concussion. Intervention studies that did not report prospective mental health outcomes for a non-intervention concussion group, studies that combined injury severities (eg, did not differentiate between concussion and mTBI/complicated mTBI) and studies that only reported mental health outcomes for children with delayed recovery were excluded. Reviews, meta-analyses, case studies, conference abstracts, book chapters, commentaries, dissertations, case reports and non-English articles were also excluded.
Eligible studies that included an orthopaedic injury or typically developing control group were included in meta-analyses, while studies that did not include a control group were included in the systematic review only (n=36).
Data classification
Mental health outcomes were restricted to the broad categories of internalising, externalising and total mental health difficulties, due to the few studies reporting findings at a disorder-specific level. The American Psychological Association endorses the utility of the internalising/externalising framework in research and clinical contexts in their introduction to the Diagnostic and Statistical Manual of Mental Disorders-fifth edition (p.13):
…clustering of disorders according to what has been termed internalizing and externalizing factors represents an empirically supported framework. Within both the internalizing group (representing disorders with prominent anxiety, depressive, and somatic symptoms) and the externalizing group (representing disorders with prominent impulsive, disruptive conduct, and substance use symptoms), the sharing of genetic and environmental risk factors, as shown by twin studies, likely explains much of the systematic comorbidities seen in both clinical and community samples.33
In keeping with the internalising/externalising framework, anxiety, depression, post-traumatic stress and withdrawal were indexed under internalising problems while aggression, conduct problems, attention problems, risk-taking and hyperactivity were classified as externalising problems.33–36 Overall mental health was measured by novel psychiatric diagnoses post-injury as well as total problem subscales of validated behavioural and emotional inventories. Pooled effect sizes were calculated for studies reporting results from multiple informants (eg, parent and child self-report) and for different outcomes underlying the same construct.
Evidence suggests that mental health changes with time post-concussion.21 However, it is unclear how internalising and externalising difficulties may evolve from very acute stages to longer term impact. We therefore included a wider range of time since injury, to capture and comment on time in the context of recovery. Existing published concussion guidelines and recovery trajectories were used to define time since injury categories. Insufficient data (n=1) were available to analyse outcomes ≤1 month post-injury. Therefore, time points were defined as follows: (1) acute: injury to <3 months post-injury, the time frame when most young people recover from concussion8 9; (2) persisting: 3–12 months post-injury, the time frame when a minority of children experience ongoing symptoms8 37; and (3) chronic: >12 months post-injury, the time frame when most novel mental health difficulties have emerged,17 reflecting the longer term impact on mental health.5 Studies were assigned to these categories using the mean time since injury at each assessed time point. Where multiple data points were measured within the same time category, results were pooled into a single effect size.
Quality assessment
The quality of eligible studies was assessed using the Downs and Black Quality Appraisal Criteria (DBC) which assigns non-intervention studies a maximum of 20 points for the highest quality across five main criteria: (a) external validity, (b) reporting, (c) bias, (d) confounding and (e) power.38 The Oxford Centre for Evidence-Based Medicine (OCEBM) 2011 Levels of Evidence were also employed as a measure of evidence strength informed by research design.39
Meta-analyses
Random effects meta-analyses were conducted using meta,40 metafor 41 and dmetar packages in R V.4.0.2.42 43 Means and SDs were used to calculate effect sizes for continuous mental health outcomes, while frequencies of events in cases and controls were used to calculate effect sizes for categorical variables. Where studies did not report adequate data to calculate effect size, the corresponding author was contacted (n=7). Studies that could not be included in the meta-analysis because appropriate data were not provided were included in the systematic review only (n=2).
Effect size was measured using Hedges’ g as it adjusts for sample size, thus providing an unbiased estimate of the standardised mean difference.44 Consistent with established recommendations for meta-analysis, effect sizes were interpreted as small (0.32), moderate (0.33–0.55) or large (>0.59).45 Heterogeneity was quantified using the I2 statistic which describes the percentage of variability in effect sizes due to heterogeneity rather than chance alone.46 Heterogeneity was interpreted as low, or unimportant (0%–30%), moderate (30%–50%), substantial (50%–80%) and considerable (80%–100%).47 Graphic Display of Heterogeneity (GOSH) plots were generated to explore patterns of heterogeneity, followed by sensitivity analyses.48 Heterogeneity was further explored through subgroup analyses and meta-regression where sufficient data were available (n≥10).49 Some prespecified analyses were unable to be conducted due to missing data (eg, premorbid mental health status) and were substituted for available alternatives (eg, exclusion of patients with psychiatric history). Influence analyses (eg, ‘leave-one-out’ approaches) were conducted to ensure that the overall estimate of the meta-analysis was not distorted by outliers or studies exerting high influence on the model.50
Results
Study selection
The study selection process is illustrated in figure 1. Sixty-nine articles representing 60 unique samples satisfied eligibility criteria and were included in the systematic review. Of these, 29 were excluded from the meta-analysis due to the absence of a control group, or because controls did not complete mental health measures, resulting in 40 articles characterising 33 unique studies included in the meta-analytical review. Characteristics and main findings of included studies are displayed in online supplemental table 2.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart.
Study characteristics
In total, 89 114 children with concussion (60.9% males) were represented in this meta-analysis. Age at injury ranged from 0 to 18 years, with a weighted grand mean of 11.69 years. Falls (42.3%) and sporting injuries (29.5%) were the most common injury mechanisms reported, followed by motor vehicle accidents (15.5%).
One-third of included studies used a prospective longitudinal design (n=20). The remaining studies used prospective cohort (n=11), cross-sectional (n=9), retrospective cohort (n=9), case–controlled (n=5), inception cohort (n=3), qualitative (n=2), retrospective chart review (n=1) and repeated measures (n=1) designs.
Assessed time points ranged from admission to 20 years post-injury. All studies used age-appropriate, validated measures of mental health (n=60), comprehensive interviews (n=2), formal psychiatric diagnoses (n=3) or engagement with mental health services (n=3) to detect mental health outcomes. The Child Behavior Checklist (n=19, 27.5%), Behavior Assessment System for Children (n=7, 10.1%) and Personality Inventory for Children (n=7, 10.1%) were the most commonly used measures. Other instruments used are listed in online supplemental table 2. Internalising problems were the most frequently assessed mental health outcomes (n=43), followed by overall mental health (n=32) and externalising problems (n=29). Parents were the most frequent respondents (n=43), followed by children (n=28) and teachers (n=7). Fifteen studies included multiple informants (parent and child, n=8; parent and teacher, n=6; parent, child and teacher n=1).
Premorbid mental health status was assessed in 28 studies (40.6%), as documented by retrospective ratings of pre-injury behaviour (n=19) or psychiatric diagnoses (n=9). Two studies employed International Classification of Disease Criteria-10, while seven studies did not specify the criteria for pre-injury mental health diagnoses. Thirty-two studies (46.3%) excluded children either with a history of mental health difficulties or hospitalisation for psychiatric illness. Twenty-one (30.4%) of the included studies did not account for pre-injury mental health status, nor exclude children with pre-injury mental health diagnoses, while 12 (17.4%) excluded pre-injury mental health diagnoses and included measures of premorbid mental health. Additional study characteristics have been outlined in online supplemental material.
Quality assessment
All included studies were rated as excellent (n=41, 61.2%) or good (n=26, 38.8%) quality on the DBC. Most included studies represented level 3 evidence according to the OCEBM Levels of Evidence (n=58, 82.9%), with seven inception cohort studies meeting criteria for level 2 (10.0%) and three studies at level 4 (4.3%). Forty-three studies (61.4%) recruited participants via consecutive admissions or inception cohort design, suggesting low risk of selection bias among most included studies. Twenty-two studies (55.0%) in the meta-analysis recruited controls from the same setting as concussion sample, suggesting risk of selection bias.
Reporting of attrition rates was fair, with 42 studies (60.9%) describing both proportion and characteristics of participants lost to follow-up. Forty-four studies reported low attrition rates (<20%) or adjusted analyses based on confounds related to patients lost to follow-up (63.8%). Fifty studies (72.5%) had clear aims and hypotheses. Five (7.2%) included power calculations. All reported key participant characteristics of patients, and the majority (n=64, 92.8%) detailed the distribution of key confounders. Of studies included in the meta-analysis, comparability between cases and controls was acceptable, with 34 (85.0%) documenting principal confounds and all studies either demonstrating no significant group differences or making adequate adjustments for confounds.
Systematic review
The results of included studies are qualitatively synthesised below, corresponding to study research questions.
How common are mental health problems after paediatric concussion?
Twenty-nine articles addressed this question. Studies consistently reported that a minority of children experienced clinically significant levels of internalising, externalising and total mental health problems after concussion16–18 28 51–59: 19.3%–40.0% of whom reported no pre-injury mental health symptoms and 50.0%–60.0% reported a history of elevated pre-injury mental health symptoms56–58 or diagnoses.17 18 Twenty-nine per cent of children with pre-injury mental health diagnoses received a novel mental health diagnosis post-concussion.17 Internalising, externalising and total mental health problems were reported within the normal range in most studies. 21 60–64 One study reported mean behaviour problems in the clinical range 3 months post-injury with resolution by 6 months.61
The prevalence of clinically significant internalising problems ranged from 3.0% to 36.7%,54 65–68 with one study reporting 40% of children demonstrated subclinical anxiety following concussion.69 Although parents reported their child’s inability to control anger among the most distressing symptoms,70 just one study reported the proportion of clinical externalising problems following concussion, at 20.0% 16 years post-injury.71 Results from a population-based study by McKinlay et al found that preschool children who attended hospital for concussion were three to four times more likely to show symptoms of attention-deficit/hyperactivity disorder, conduct disorder, oppositional defiant disorder, substance abuse and mood disorder during early adolescence, compared with typically developing controls and children who presented to outpatient services after concussion.28 51
What factors predict mental health following paediatric concussion?
Studies reported several factors influenced mental health after paediatric concussion (n=28). Pre-injury mental health was consistently identified as a strong predictor of post-injury mental health problems.16 17 57 66 72 73 Five studies systematically examined this relationship with regression analyses and demonstrated that psychiatric history explained between 38.4% and 65.0% of variance in mental health problems post-concussion.16 17 66 73 74 Age and sex were inconsistent predictors of mental illness. Internalising vulnerabilities were associated with female sex21 22 52 75–77 and older age at injury.17 21 60 61 78 Females appeared at greater risk of developing novel mental health difficulties after concussion,21 52 75 76 but this finding was not universal.17 55 Males with a psychiatric history were at increased risk of developing further psychiatric illness after concussion.17 Younger age at injury was associated with more externalising problems17 22 and post-traumatic stress symptoms,76 however some studies found no association between age and mental health or psychosocial functioning.65 69 While several studies indicated a role for family factors,17 18 52 57 68 79 80 only five studies explored family characteristics post-concussion.16 22 72 80 81 Results showed that family functioning, parent mental health, parent distress and family characteristics (eg, family living arrangement, parent education) were associated with externalising problems 6 months after concussion.16 22 72 80 81 In contrast, family characteristics did not predict internalising problems above and beyond participant characteristics.16
Two studies explored protective factors associated with better mental health outcomes, identifying positive family environment, cultural and psychological resilience as associated with better quality of life and lower levels of depression, anxiety, adjustment and attention-deficit/hyperactivity symptoms.22 75
How does mental health interact with recovery from concussion?
Few studies directly examined the interaction between mental health and PCS (n=11). Internalising symptoms significantly predicted acute and post-acute PCS.5 75 82 Higher premorbid PCS predicted increased psychological difficulties over time.52 73 Nonetheless, even when taking pre-injury data into account, considerable variation in recovery trajectories exists.56
How does mental health change with time post-injury?
In the nine studies addressing this issue, mental health symptom profile tended to remain stable over time,69 with most novel psychiatric diagnoses developing in the first-year post-concussion.17 Significant improvements in mental health emerged between 3 and 6 months post-injury.21 72 83 Among infants and toddlers, social and emotional behaviour worsened over time,84 with significantly higher rates of conduct, oppositional defiant, attention-deficit/hyperactivity, substance use and mood disorder symptoms evident several years post-concussion.28
Meta-analyses
We then conducted meta-analyses to determine if children experienced elevated mental health difficulties after concussion compared with controls.
Internalising problems
Significant, moderate effects were observed in the concussion group compared with controls across acute (t=5.12, g=0.45, 95% CI (0.17 to 0.74), p=0.01) persisting (t=4.26, g=0.42, 95% CI (0.20 to 0.63), p=0.001) and chronic (t=2.88, g=0.41, 95% CI (0.10 to 0.72), p=0.01) outcomes (see figure 2). At each time point, there was a large prediction interval and low to considerable heterogeneity (acute: I2=0.0%, 95% CI (0.0% to 76.8%), Q(3)=1.98, p=0.58; persisting: I2=51.0%, 95% CI (5.3% to 74.7%), Q(11)=22.46, p=0.02; chronic: I2=49.3%, 95% CI (6.2% to 72.6%), Q(13)=25.67, p=0.02). GOSH diagnostics identified outliers contributing to cluster imbalance in both persisting (n=2) and chronic models (n=4). Pooled estimates remained significant omitting these outliers and heterogeneity was low to moderate (persisting: g=0.46, 95% CI (0.32 to 0.59), p<0.0001, I2=36.1%; chronic: g=0.27, 95% CI (0.11 to 0.42), p=0.003, I2=28.9%; online supplemental figure 1). Leave-one-out analyses revealed that all pooled estimates after excluding one study at a time fell within the 95% CI of the overall estimate. Funnel plots and Egger’s test showed evidence of publication bias in chronic internalising outcomes (p=0.003). Nonetheless, p-curve analyses supported evidential value suggesting that a true effect size underlies presented findings and that results are not the product of publication bias and p-hacking alone.
Supplemental material

Standard mean difference (SMD), treatment effect (TE) and standard error (seTE) of acute, persisting and chronic internalising problems after paediatric concussion.
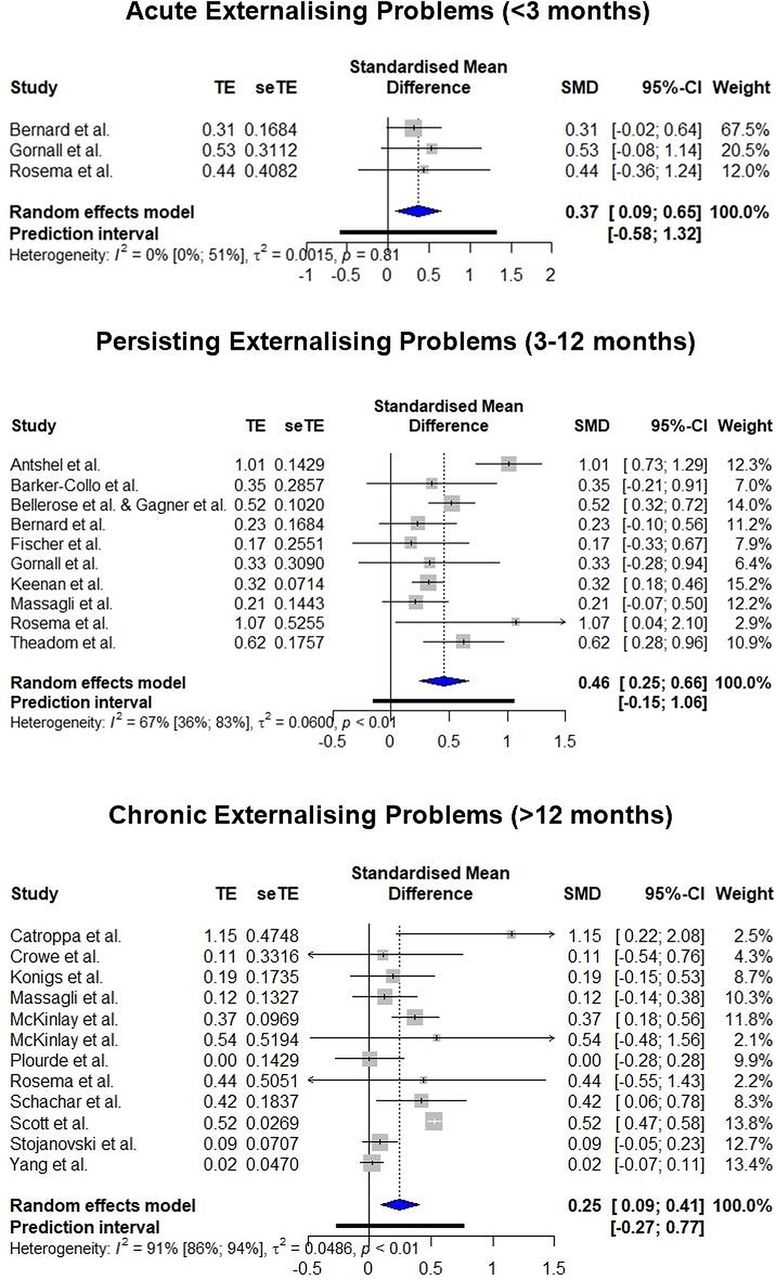
Externalising problems
Significant, moderate effect sizes were observed across acute (t=5.77, p=0.03, g=0.37, 95% CI (0.09 to 0.65)) and persisting (t=4.94, p<0.001, g=0.46, 95% CI (0.25 to 0.66)) time points, decreasing to a small effect in the chronic model (t=3.46, p=0.005, g=0.25, 95% CI (0.09 to 0.41); see figure 3). Heterogeneity was low to moderate and non-significant for acute externalising problems (I2 =0.00%, 95% CI (0.00% to 50.5%), Q(2)=0.42, p=0.81) but substantial and significant among studies investigating persisting (I2=66.9%, 95% CI (35.5% to 83.0%), Q(9)=27.18, p=0.001) and chronic effects (I2=90.7%, 95% CI (85.7% to 94.0%), Q(11)=118.32, p<0.0001). GOSH diagnostics identified outliers contributing to cluster imbalance in both persisting (n=3) and chronic models (n=3). We reperformed the meta-analyses omitting outliers and the pooled estimates remained significant with low heterogeneity (g=0.38, 95% CI (0.21 to 0.54), p=0.001, I2=8.4%; g=0.19, 95% CI (0.07 to 0.32), p=0.007, I2=18.8%; online supplemental figure 2). Leave-one-out analyses revealed that all pooled estimates after excluding one study at a time fell within the 95% CI of the overall estimate. No evidence of publication bias was identified on funnel plots or Egger’s test. Evidential values supported a true effect size underlying present results.
Supplemental material

Standard mean difference (SMD), treatment effect (TE) and standard error (seTE) of acute, persisting and chronic externalising problems after paediatric concussion.
Total problems
Significant, small to moderate effects were observed across acute (t=7.34, p=0.02, g=0.49, 95% CI (0.20 to 0.78)), persisting (t=3.24, p=0.01, g=0.28, 95% CI (0.08 to 0.49)) and chronic total mental health problems (t=3.91, p=0.005, g=0.22, 95% CI (0.09 to 0.35)), with effect size decreasing over time (see figure 4). Heterogeneity was low to moderate and non-significant across the acute (I2=0.00%, 95% CI (0.00% to 51.4%), Q(2)=0.43, p=0.81) and chronic time points (I2=20.7%, 95% CI (0.00% to 62.0%), Q(8)=10.09, p=0.26), but moderate to high in the persisting model (I2=66.7%, 95% CI (29.6% to 84.3%), Q(7)=21.03, p=0.004). GOSH diagnostics identified outliers contributing to cluster imbalance in both persisting (n=2) and chronic models (n=1). We reperformed meta-analyses omitting outliers, and pooled estimates remained significant with low heterogeneity (g=0.38, 95% CI (0.26 to 0.49), p=0.0004, I2=0.0%; g=0.18, 95% CI (0.08 to 0.29), p=0.004, I2=9.4%; online supplemental figure 3). Leave-one-out analyses revealed that all pooled estimates after excluding one study at a time fell within the 95% CI of the overall estimate. Chronic, but not persisting, outcomes showed evidence of publication bias on funnel plot and Egger’s test (p=0.02); however, evidential values supported a true underlying effect.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Standard mean difference (SMD), treatment effect (TE) and standard error (seTE) of acute, persisting and chronic total mental health problems after paediatric concussion.
Additional analyses
Meta-analyses stratified by age and sex were not possible due to the lack of age-specific and sex-specific data reported in the included studies. Meta-regressions evaluating the impact of sex (% males) and age (mean age) on mental health were, therefore, conducted. Variability in persisting internalising and externalising outcomes was not explained by any of the demographic or methodological factors examined (see online supplemental tables 2 and 3). Chronic internalising problems significantly differed by OCEBM Level of Evidence, with level 3 studies showing the greatest effect size (g=0.51), followed by levels 4 (g=0.38) and 2 (g=0.10). Sex and DBC quality rating accounted for 7.78% and 5.63% of variance, respectively, but were non-significant predictors overall. In the chronic externalising model, mean age accounted for 5.00% of variance, but was a non-significant predictor overall. As with persisting outcomes, no other factors significantly accounted for heterogeneity at the chronic time point. Insufficient studies were available to conduct subgroup analyses or meta-regressions on total behaviour problems. Online supplemental figures 4–7 present forest plots by design and respondent.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Discussion
The aim of our paper was to systematically investigate mental health outcomes following paediatric concussion while controlling for key methodological differences that have limited synthesis of paediatric concussion research. Our results revealed that mental health is highly relevant to concussion recovery. Both the qualitative synthesis and meta-analysis demonstrated that, even among studies with homogeneous designs, samples and concussion definitions, mental health outcomes can vary widely. This indicates that children respond to concussion in diverse ways. While mental health generally improves with time post-injury, a minority of children experience clinically significant and persisting mental health symptoms that warrant clinical attention. Post-traumatic stress and depressive symptoms in particular have been associated with increased risk for adverse outcomes after concussion.54 85 Evidence suggests that pre-existing mental health symptoms, family anxiety, the psychosocial impact of post-concussion symptoms and reduced activity may contribute to ongoing mental health symptoms in this group.16 17 57 66 72 73 86–88 Despite this chronic vulnerability, only a small proportion of children access mental healthcare after concussion,52 59 highlighting this as a missed opportunity for early intervention.
In contrast to recovery from PCS more generally,8 few studies reported significant improvements in mental health symptoms by 1 month post-injury,83 suggesting that mental health symptoms may take longer to resolve than other post-concussion symptoms. This suggests that concussion is an important factor precipitating subsequent mental health symptoms, which may be maintained by biopsychosocial factors related to concussion (eg, fatigue) and context (eg, worry about repeat injury). Of note, the most commonly employed measures of PCS include symptoms that overlap considerably with mental health (eg, emotional lability, irritability, nervousness, sadness), leading to difficulties differentiating PCS and mental health symptoms.89 Despite this confound, few studies commented on the potential overlap in measurement of these two dimensions. This relationship may be driven by a high level of symptom overlap between PCS and mental health difficulties, or by a feedback loop where persisting PCS precipitate acute stress which then exacerbates mental health symptoms, which further impacts PCS.
The less competitive nature of sport among younger children contributes difficulties differentiating sport from non-sport concussion in paediatrics. Therefore, little research has been conducted on sport concussion in children under 13 years,9 despite a significant proportion of paediatric concussions sustained during sport.90 Sport-concussion research is important given the increased risk of repeated concussions,9 which has been associated with mental health difficulties and delayed recovery.4 14 Results from this review highlight that mental health outcomes from sport53 77 82 91 and non-sport concussion are broadly consistent, despite greater representation of older children and adolescents in sport concussion research. While clinical recommendations for non-sport-related concussions are lacking, these findings highlight that, alongside clinical judgement, sport-related concussion guidelines are likely to be highly relevant to the assessment and management of non-sport concussion.
Current evidence establishes pre-injury mental health difficulties as the strongest and most consistent predictor of post-concussion mental health outcomes; however, novel diagnoses occur in approximately one-third of young people after concussion.17 Female sex was associated with increased internalising problems after concussion, however, this vulnerability is also evident in the general population and is unlikely to be concussion specific. Age was an inconsistent predictor of mental health outcomes. Interaction effects between age and sex are a potential explanation for this variability with internalising problems increasing with age among females.21 Given that female sex and older adolescence have also been identified as risk factors for delayed recovery following concussion,4 present results may reflect vulnerability to adverse outcomes from concussion more broadly, the emergence of mental health difficulties observed among females during adolescence, or an interaction between these factors and their psychosocial context.
Infants and toddlers may also experience social and emotional difficulties that worsen over time,84 with significantly higher rates of conduct, oppositional defiant, attention-deficit/hyperactivity, substance use and mood disorder symptoms evident several years post-concussion.28 This finding might be explained by the fact that younger children are less likely to have existing mental health diagnoses, reflect developmentally specific neurobehavioural outcomes, family anxiety, incidental reinforcement of maladaptive coping (eg, reassurance seeking, separation anxiety) or a combination of these factors. Further research is needed to explore the relationship between concussion, mental health and child development in greater detail.
Psychological resilience and family characteristics emerged as promising, but largely unexplored, predictors of post-concussion mental health outcomes. Given these domains offer the potential for early intervention, further exploration of these factors may provide opportunities to improve mental health outcomes.
Consistent with reviews of elite collegiate athletes,92 our results support an association between concussion and acute internalising mental health symptoms. While depressive symptoms in elite collegiate athletes resolve within 1 month post-concussion,92 our review suggests that both internalising and externalising problems persist longer in children and adolescents. Such long-term mental health problems have also been highlighted in a narrative review of suicidality after concussion and mTBI among children, adults and military personnel, showing a twofold greater risk of suicide compared with peers.93 Our review extends our understanding of mental health consequences of concussion to children and adolescents, who may be at greatest risk of adverse outcomes.9
This systematic review and meta-analysis included studies employing a variety of designs, providing an opportunity to explore the impact of research design on study results. Prospective cohort and longitudinal prospective cohorts generally found larger effects than cross-sectional, case–control, retrospective cohort and inception cohort designs. This may reflect bias in reporting positive results or strengths of prospective cohort designs, including accuracy of data collection regarding exposures, confounders and timing of concussion. Population studies often revealed long-term impacts that were not evident in many retrospective designs.59 65 94–96 Consistent with population data,27 28 51 78 97 several prospective longitudinal cohort studies reported increased mental health difficulties several years post-concussion.15 16 57 62 71 75 98
Clinical implications
Results from our review highlight the importance of considering mental health as a predisposing, exacerbating and protective factor for concussion recovery. Findings that PCS subtypes are relatively stable over time since injury17 69 highlight the potential and importance of early intervention. When making recommendations for concussion management, clinicians should consider potential mental health consequences, particularly where premorbid mental health difficulties are present.
Previous management approaches, such as prolonged rest, have been associated with poor mental health and adverse outcomes after concussion.87 88 Current clinical guidelines for recovery support a systematic and graduated return to exercise, school and sport.9 99 100 The CISG Berlin Consensus Statement outlines the importance of applying this protocol alongside clinical judgement, on an individual basis.9 The statement further highlights the utility of structured interventions, such as graded exercise101 and physiotherapy tailored to individual symptoms.102 103 Less is known about treatment of mental health symptoms, with initial promise shown with the use of cognitive–behavioural paradigms,104 either alone or as part of collaborative care models. The trajectories of PCS and mental health symptoms are closely intertwined among children with delayed recovery,105 further demonstrating mental health as an important target for intervention.
Since the majority of children and adolescents with clinical mental health difficulties do not access recommended care,106 incorporating mental health risk into post-injury management represents an avenue to engage young people with mental health services to either prevent unnecessary problems emerging or to treat premorbid issues.
The presence of psychological distress is associated with twice the healthcare costs after paediatric concussion,107 further highlighting the importance of early intervention. When assessing persisting post-concussion symptoms, clinicians should be cognisant of the potential overlap between PCS and mental health symptoms. As a first step, mental health should be evaluated as part of standard acute concussion assessment and management. This may encourage families to monitor and seek support for emerging or exacerbated emotional and psychological symptoms. Among children with delayed recovery, parent anxiety contributes additional family burden following childhood concussion, indicating a need for management strategies to consider the implications to the entire family.86
Anxiety and depression significantly mediated the relationship between resilience and post-concussion symptoms,108 suggesting that mental health has an important impact on recovery from concussion, even accounting for individual characteristics. While children provided different reasons for their emotional distress (eg, inability to play sport, others’ lack of understanding about concussion), they consistently reported frustration, depression, anxiety, irritability and feelings of isolation associated with their injury.91 Considered together, current evidence supports the use of a biopsychosocial model for understanding the factors contributing to the development and maintenance of mental health difficulties post-concussion on an individual basis.
Strengths and limitations
This systematic review extends past literature by focusing specifically on mental health after concussion in a paediatric population and is among the first to perform a meta-analysis. Major strengths are precise inclusion criteria, thorough search strategy and robust evaluation. Nonetheless, several limitations need to be acknowledged. First, we excluded unpublished and non-English language articles, which may subject findings to publication and language bias. Although risk of publication bias was identified for some comparisons, further analyses supported the presence of a true effect underlying results. This systematic review and meta-analysis included studies employing a variety of designs, assessment tools and respondents. While this can increase heterogeneity, it also provides an important opportunity to comment on the impact of research design on mental health outcomes and focus of past research. To balance these considerations, we restricted inclusion to studies that measured mental health prospectively, regardless of how other unrelated measures were obtained. Considering the relatively small number of studies and the results of subgroup analyses conducted, the impact on the overall conclusions is minimal.
Limitations of the literature
At a study level, only four studies explored mental health outcomes within the first 3 months of concussion. Forty-one studies (59.4%) addressed mental health as the primary outcome. In the remaining studies, mental health was a secondary consideration to cognition (n=11), physiology (n=10), sleep (n=3) or quality of life related (n=4). Only two studies separated mental health data by sex and age group, highlighting significant gaps in past research and limiting the generalisability of acute findings.
Pre-injury mental health was reported in less than half of the included studies. While most of these studies employed a validated measure of pre-injury mental health, few reported the criteria for formal diagnosis. Most studies relied on normed and validated parent or self-report mental health measures. While child respondents generally reported more mental health difficulties than parents and diagnoses reported in medical records, results were broadly consistent across studies. Studies including multiple respondents showed lower variability than single respondents highlighting valuable increase in precision. Finally, although 69 studies were identified as eligible for the systematic review, nearly half of these were excluded from the meta-analysis due to the absence of a control group.
Future directions
Future studies seeking to address design limitations should aim to assess pre-injury mental health, incorporate clinical assessment and include multiple respondents with a robust, clearly defined measure of pre-injury mental health. Reporting age-specific and sex-specific results will clarify the relationship to mental health outcomes highlighted in this review. Methodology would be strengthened by including a control group, reporting power analyses and continuing to minimise bias wherever possible. The complex relationship between mental health and concussion recovery requires further study, with particular attention focused on the role that personality, resilience, family, developmental and environmental factors may play in mental health after paediatric concussion. In-depth clinical interviews and qualitative research designs, largely lacking to date, are needed to extend these quantitative findings and draw out these complex relationships. To date, many studies have excluded children with a history of mental health diagnoses. Given the community prevalence of mental illness among children and adolescents and the potential role that mental health may play in recovery from concussion, this represents an important limitation, which likely skews our current understanding of concussion recovery and its underlying mechanisms. Mental health was predominantly reported by parents, with only a quarter of studies including multiple informants. Given that parents’ understanding of concussion may influence their perceptions and attributions of post-injury mental health difficulties,80 future research should obtain a range of perspectives.
Conclusions
Our study revealed that children experience elevated mental health difficulties after concussion which can persist several years post-injury. Assessment, prevention and intervention of mental health difficulties after concussion should be integrated into standard concussion management. A range of biopsychosocial factors need to be considered to clarify the nature of post-concussion recovery on an individual basis. Further research is needed to illuminate the mechanisms underlying observed relationships between mental health, PCS and psychosocial factors.
What is already known?
Concussion is a common injury among children and adolescents.
While some studies report significant mental health problems after childhood concussion, other studies report no such finding.
Several post-concussion symptoms overlap with mental health symptoms, however, the relationship between delayed recovery and mental health remains poorly understood.
What are the new findings?
Mental health is highly relevant to concussion recovery, although the ways children respond to concussion are diverse.
A minority of children experience clinically significant mental health symptoms that warrant clinical attention, particularly in the presence of post-traumatic stress symptoms and depression.
Current evidence establishes pre-injury mental health difficulties as the strongest and most consistent predictor of paediatric post-concussion mental health outcomes, however, novel diagnoses occur in approximately one-third of young people after concussion.
Psychological resilience and family characteristics are promising, but largely unexplored, predictors of post-concussion mental health outcomes.
In contrast to recovery from post-concussion symptoms more generally, mental health symptoms may take longer than 1 month to resolve.
Current evidence supports the use of a biopsychosocial model for understanding the factors contributing to the development and maintenance of mental health difficulties post-concussion on an individual basis.
How might it impact on clinical practice in the future?
Mental health should be evaluated as part of standard paediatric concussion assessment and management in the context of biopsychosocial factors.
Mental health should be considered a potential predisposing, exacerbating and protective factor for paediatric concussion recovery.
When making recommendations for concussion management in children, clinicians should consider potential mental health consequences, particularly where premorbid mental health difficulties are present.
Incorporating mental health risk into post-injury management represents an avenue to engage young people with mental health services to either prevent unnecessary problems emerging or to treat premorbid issues.
When assessing persisting post-concussive symptoms in children, clinicians should be cognisant of the potential overlap between post-concussive symptoms and mental health symptoms.
Ethics statements
Acknowledgments
The authors would like to thank all researchers who provided additional data for inclusion in this meta-analysis and the librarian, Poh Chua, from the Royal Children’s Hospital for her assistance in designing the search strategy used in this review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @VickiAn28323584
Contributors AG designed the search strategy, conducted the systematic searches, completed title, abstract and full-text screening, completed quality analysis, conducted meta-analyses and qualitative synthesis, and drafted the manuscript. TM co-screened title and abstracts for this review. XL co-conducted the full-text review. MT completed quality analysis consensus and critically revised the manuscript for important intellectual content. VA contributed to the conception of this study and critically revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This research was supported by the Victorian Government Operational Infrastructure Scheme. MT is funded by a research grant from the Royal Children’s Hospital Foundation. VA is funded by an Australian National Health and Medical Research Council Senior Practitioner Fellowship. This research was conducted as part of AG’s PhD research which is supported by the Australian Government Research Training Scheme.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.