Article Text

Abstract
Objective Investigate whether exercise-based telerehabilitation improves pain, physical function and quality of life in adults with physical disabilities.
Design Systematic review of randomised controlled trials.
Data sources Searches were performed in AMED, MEDLINE, CINAHL, SPORTDiscus, Embase, PEDro, Cochrane Library and PsycINFO.
Eligibility criteria Trials were considered if they evaluated exercise by telerehabilitation. The population included adults with physical disability. Comparisons were control and other interventions. The outcomes were pain, physical function and quality of life. Study selection, data extraction and analysis followed the protocol registered in PROSPERO (CRD42019122824). GRADE determined the strength of evidence.
Results Forty-eight trials were included in the quantitative analysis. When compared with other interventions, there was high-quality evidence that telerehabilitation was not different to other interventions for pain (95% CI: −0.4 to 0.1), physical function (95% CI: −0.2 to 0.2) and quality of life (95% CI: −0.1 to 0.5) at long-term. There was moderate-quality evidence that telerehabilitation was not different to other interventions for physical function (95% CI: −0.1 to 0.5) and quality of life (95% CI: −0.2 to 0.5) at short-term. However, due to the low-quality evidence and the small number of trials comparing exercise protocols offered by telerehabilitation with control groups, it is still not possible to state the efficacy of telerehabilitation on pain, function and quality of life at short-term and long-term.
Conclusions Exercise by telerehabilitation may be an alternative to treat pain, physical function and quality of life in adults with physical disabilities when compared with other intervention.
- exercise rehabilitation
- disability
- physical activity
- quality of life
Statistics from Altmetric.com
Introduction
According to the World Report on Disability (WHO 2011), over one billion people live with a disability worldwide, and almost 200 million experience considerable functional limitations.1 Healthcare services face challenges to address the needs of people with physical disabilities,2 including: patients’ physical incapacity to attend treatment centres, absence of caregivers, scarcity of health professionals and limited resources in local communities. Lack of transport to clinical centres can be a particular barrier for people with disability to access care.1 3 4 Limited access to healthcare services may allow health and quality of life to deteriorate.5
To address these challenges, many countries are employing telecommunication technologies as part of the healthcare service.6 Telerehabilitation may improve the quality of services by monitoring patients in their own place, mainly in communities far from urban centres. It is also expected to improve cost-effectiveness of interventions.7–9 Previous systematic reviews have evaluated the feasibility, efficacy and cost of telerehabilitation for people with different health conditions, and the reviews supported telerehabilitation as an effective alternative to supervised/face-to-face interventions.10–13
Exercise is one of the treatments that clinicians can deliver using telerehabilitation. Exercise is cost-effective14 15 and recommended for people with physical disabilities due to musculoskeletal conditions, coronary heart disease, some types of cancer, type 2 diabetes, hypertension, among others.16
Conclusions from previous systematic reviews that investigated effectiveness of exercise by telerehabilitation in people with physical disabilities were limited by confounders such as inclusion of poor quality studies (ie, no randomised controlled trials),17 18 and absence of investigation of effect sizes and the strength of the recommendation.18 The aim of this systematic review of randomised controlled trials was to investigate short-term and long-term effectiveness of exercise by telerehabilitation on pain, physical function and quality of life in adults with physical disabilities when compared with control and other interventions. Effect estimates and a rating of the certainty of the current evidence were reported.
Methods
Search strategy and inclusion criteria
The present systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)19 and Cochrane recommendations.20 Its protocol was prospectively registered at PROSPERO (CRD42019122824). Search strategies were conducted in May 2018 and updated in February 2020 on Allied and Complementary Medicine Database (AMED), Medical Literature Analysis and Retrieval System Online (MEDLINE), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Excerpta Medica dataBASE (Embase), Physiotherapy Evidence Database (PEDro), Cochrane Library, SPORTDiscus and PsycINFO database. There was no date or language restriction. Online supplemental material 1 details the search strategy. The health condition of interest was unlimited to increase sensitivity of our search strategy, avoiding exclusions of potential populations that we were unaware of. In addition, we manually searched identified systematic reviews in the area and specific journals of telemedicine (eg, Journal of Telemedicine and Telecare, and Telemedicine Journal and e-Health) to identify potentially relevant trials.
Supplemental material
We included published randomised controlled trials investigating effectiveness of telerehabilitation on pain, physical function and/or quality of life in adults with physical disabilities. Physical disability was defined according to the International Classification of Functioning, Disability and Health (ICF). In the ICF, issues with human functioning are categorised in three interconnected components: impairments are issues in body function or alterations in body structure; activity limitations are issues in executing activities; participation restrictions are issues involving any area of life. Physical disability refers to difficulties encountered by people with health conditions in any or all three components of functioning described above.21
Population of interest were adults (≥18 years old) with physical disabilities related to any health condition. Telerehabilitation was considered in the current review as any take-home exercise (ie, aerobic exercises and/or kinesiotherapy) provided by telecommunication technologies such as phone calls, video conferences and/or software applications.7 We arbitrarily decided to exclude trials investigating virtual reality by telerehabilitation because of the specificity of the theme and costs of the technology. Comparators of interest were control (ie, no intervention, waiting list, placebo or sham) and other interventions (ie, any other active intervention such as traditional rehabilitation at home or in healthcare facilities). Our outcomes of interest were pain, physical function and quality of life. Trials were included if they reported any valid measures of our outcomes of interest such as: Visual Analogue Scale (VAS) or Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale for pain;22 6 min walk test (6MWT) or Arthritis Self-Efficacy Scale (AIMS2) subscale for physical function;23 and Short Form Health Survey-36 (SF-36_ or Minnesota Living with Heart Failure questionnaire for quality of life.24 When more than one valid measure was available in the trial for the same outcome, we considered the most consistent measurement instrument across trials included in this review.25–73
Study selection
After searches, retrieved references were exported to the EndNote Reference Manager Software and duplicates were removed. Then, titles and abstracts were screened, and two reviewers independently (JFD and FCMSD) assessed potential full-texts using our eligibility criteria outlined above. Trials fulfilling our eligibility criteria were included in the review. A third reviewer (RFS) solved disagreements.
Two reviewers independently (JFD and PRTB) assessed the quality of included trials using the 0 to 10 PEDro scale (http://www.pedro.org.au/). The PEDro scale has been shown to have acceptable reliability and validity for rating quality of randomised controlled trials.74 75 A third reviewer (RFS) solved discrepancies. When available, we used the scores from the PEDro database.76
Data extraction
The two reviewers independently (JFD and PRTB) extracted descriptive and outcome data from included trials, and the third reviewer (RFS) solved discrepancies. Descriptive information included: source of participants; health condition; age; sex; type and dosage for telerehabilitation and comparators; outcomes; and time points. Extracted outcome data included means, standard deviations (SDs) and sample sizes of all groups to investigate short-term and long-term effects. Short-term effect was considered follow-up up to 3 months after baseline, and long-term effect was considered follow-up over 3 months after baseline. When more than one time point was available within the same follow-up period, the one closer to the end of the intervention was considered. If trials investigated more than one type of exercise by telerehabilitation31 or more than one comparator,29 40 groups were combined as recommended by Cochrane.77 Some included trials did not provide SDs and data were imputed from: SEs;26 CIs;29 46 P values;46 65 medians and IQRs;36 44 61 64 or other trials included in the review that used the same instrument,37 following the Cochrane recommendations.77 Trials that reported outcome data not normally distributed (ie, mean/SD ratio of less than 2)78 and did not provide log-transformed outcome data29 31 40 48 56–58 68 72 73 were excluded from the quantitative analyses (ie, meta-analyses), following recommendations.77 Online supplemental material 2 details the data extraction.
Supplemental material
Study analysis
Meta-analysis was conducted using random-effects model because of the effects being estimated in the different studies were not identical. The model represents our lack of knowledge about why real or apparent intervention effects differ by considering the differences as if they were random.77 For the outcomes of interest, standardised mean differences (SMDs) and 95% CIs were presented, at first, for overall effect analyses on pain, physical function and quality of life in the forest-plots. The overall effects of telerehabilitation in people with physical disabilities (all health conditions combined) investigated the efficacy of telerehabilitation on outcomes of various functional levels. We chose to do this overall analyses as people with different health conditions may experience similar difficulties across functional levels.79 After the overall analyses, subgroup analyses investigated potential impact of specific clinical categories. Trials were categorised following the International Classification of Diseases and Related Health Problems (ICD-10) and grouped into 10 clinical categories (oncology, neurology, cardiovascular, pulmonary, urology, musculoskeletal, postoperative orthopaedic conditions, rheumatological, endocrine and multiple conditions).80 Subgroup and sensitivity analyses assessed potential sources of heterogeneity: clinical categories; and methodological quality of included trials (ie, a PEDro score <6 out of 10 was considered poor quality), using meta-regression when possible (ie, when at least 10 trials were pooled, following the Cochrane recommendations).77 Otherwise, qualitative subgroup analyses were conducted by different clinical categories and removing poor quality trials (ie, when less than 10 trials were pooled). Publication bias was investigated using the funnel plot and the Egger’s test when at least 10 trials were pooled.81 All analyses were conducted using Comprehensive Meta-analysis software, V.2.2.04 (Biostat, Englewood, New Jersey). Estimated effect sizes were assessed using Cohen’s benchmarks: d≥0.2 for small; d≥0.5 for medium; and ≥0.8 for large effects.82
The two reviewers independently (JFD and PRTB) assessed the strength of the recommendation using the GRADE system.83 According to the four-level GRADE system, recommendation may range from high to very-low quality. Low levels indicate uncertainty of the estimated effects. In the current review, high-quality evidence was downgraded in one point for each of the following issues: imprecision when analysed sample <400;84 risk of bias when >25% of the participants were from trials with a high risk of bias (ie, PEDro score <6 out of 10);85 inconsistency when I2 statistics >50% or when pooling was not possible;86 and publication bias when pooling ≥10 trials.81 A third reviewer (RFS) solved discrepancies between reviewers.
Results
Study selection
We identified 8205 references and 60 original trials were included in the review. The main reasons for exclusion of potential full-texts were: no population of interest (n=13); no intervention of interest (n=100); no comparator of interest (n=9); no outcome of interest (n=17); and not published randomised controlled trials (n=26). The flowchart describing trials selection is in figure 1.

Flow of studies through the review (n=60 original trials included in qualitative synthesis and n=50 original trials included in quantitative synthesis). LT, long-term; ST, short-term.
Study characteristics
Characteristics of included trials and outcome data are presented in online supplemental material 3. All 60 included trials were published between 2002 and 2019. They were conducted in Europe (n=20, 33.3%), North America (n=17, 28.3%), Oceania (n=10, 16.6%), Asia (n=10, 16.6%), Africa (n=2, 3.3%) and South America (n=1, 1.6%). Thirteen trials were conducted in USA and 10 in Australia. In 76% of the trials (n=46), a single technological resource was used as telerehabilitation (eg, video or telephone). The others combined more than one technology (eg, video and telephone, n=4, 6.7%; video, telephone and audio, n=2, 3.3%; Internet-based and telephone, n=2, 3.3%).
Supplemental material
All telerehabilitation exercise programmes included in this review were home-based. The duration ranged from 10 days to 12 months, with weekly frequency and duration of each session ranging from 2 to 7 times and from 20 to 90 min, respectively. Programmes included strength and stretching exercises combined or not with aerobic exercise. Initial evaluation of participants was conducted in all trials. After the initial evaluation, six trials35 45 53 57 71 87 had initial face-to-face contact with participants to establish goals, performed the supervised exercise programme and verified the correct use of telerehabilitation devices. Eight trials27 28 34 43 44 51 65 88 adopted face-to-face meetings with the telerehabilitation group during the intervention period to conduct sessions supervised by therapists and verified the absence of complications.
Seven trials with 898 participants compared telerehabilitation with control (ie, no intervention, waiting list, placebo or sham),25 31 32 52–54 72 and 53 trials including 4920 participants compared telerehabilitation with other interventions (ie, traditional rehabilitation at home or in healthcare settings, gym-base exercises, written programmes, usual care-medications and oxygen prescription, medical and other professionals follow-up and encouragement to improve physical activity).26–30 33–51 55–71 73 89–93 Forty one trials reported short-term effects (ie, ≤3 months after baseline) and 19 reported long-term effects (ie, >3 months after baseline). Pain, physical function and quality of life were investigated in 23, 55 and 37 trials, respectively.
Quality of the methods in the included trials
The quality of the methods in the included trials ranged from 4 to 8 points on the 0 to 10 PEDro scale (table 1). All trials reported random allocation, differences between groups, point measures and measures of variability. Forty (66.6%) out of the 60 included trials scored above 6 points on the PEDro scale. The main reasons for downgrading the methodological quality were lack of therapist blinding (n=60, 100%), lack of participant blinding (n=60, 100%), lack of concealed allocation (n=30, 50%) and absence of intention-to-treat analysis (n=29, 48%).
Methodological quality of the included trials using the 0 to 10 PEDro scale. (n=60 original trials). *Trials included in the quantitative analysis (n=50)
Effects of telerehabilitation on pain, physical function and quality of life
We presented our quantitative findings by outcome of interest (data from 50 trials). First, we report the overall effect analyses of telerehabilitation in people with physical disabilities (all health conditions combined) (figure 2). We then categorise effects by subgroups of health conditions categorised according to the ICD-10 were estimated (figure 3). In the overall effect analyses, evidence was downgraded due to risk of bias (PEDro score <6) and /or inconsistency (I²>50%). We found no evidence of publication bias (ie, Funnel plots and Egger’s tests when pooling at least 10 trials are provided in online supplemental material 4).
Supplemental material
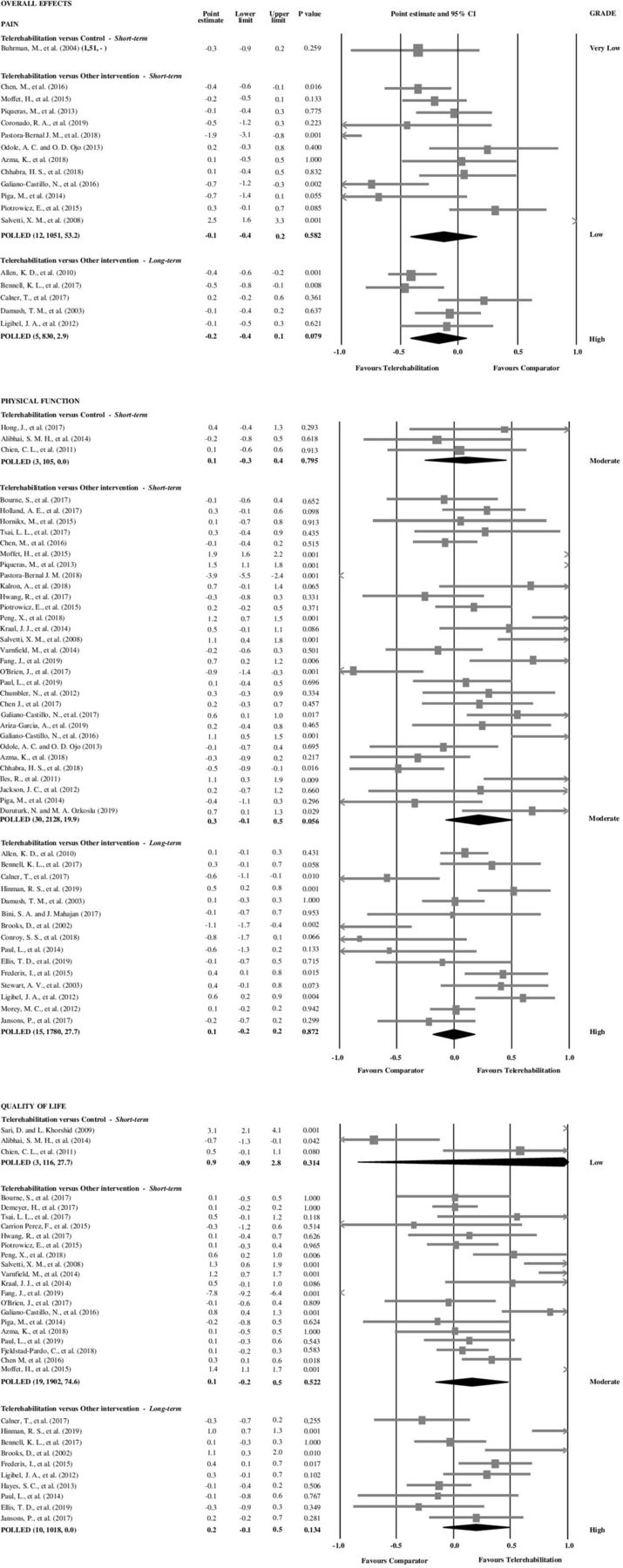
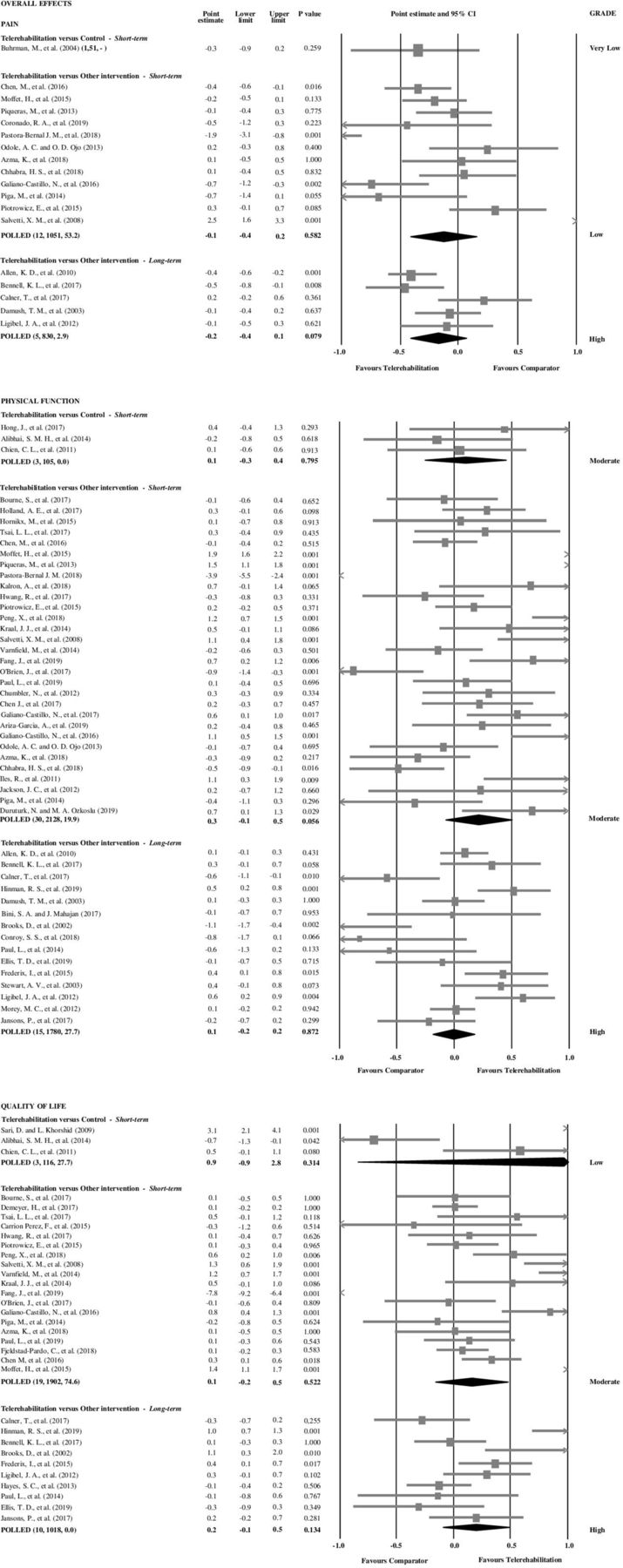
Overall effects of telerehabilitation on pain, physical function and quality of life. In parentheses: number of trials, total number of participants, I². Pain other intervention short-term: (Z=−0.5, random-effects). Pain other intervention long-term: (Z=−1.8, random-effects). Function control short-term: (Z=0.3, random-effects). Physical function other intervention short-term: (Z=1.9, random-effects). Physical function other intervention long-term: (Z=0.2, random-effects). Quality of life control short-term: (Z=1.0, random-effects). Quality of life other intervention short-term: (Z=0.8, random-effects). Quality of life other intervention long-term: (Z=1.5, random-effects). Pain control short-term: individual trial.

{kind=link}
{kind=link}
{kind=link}
Subgroup analyses by clinical categories for pain, physical function and quality of life. In parentheses: number of trials, total number of participants, I².
Overall effects (all health conditions were combined) of telerehabilitation on pain, physical function and quality of life
Pain
In the overall effect analyses for pain at long-term, there was high-quality evidence that telerehabilitation was not different to other interventions (SMD: −0.2; 95% CI: −0.4 to 0.1 p=0.079; five trials27 28 30 46 47; n=830 participants). At short-term, the strength of the recommendation was low and very low when telerehabilitation was compared with control and with other intervention (figure 2).
Physical function
Overall effect analyses showed high-quality evidence that telerehabilitation was not different to other interventions on physical function at long-term (SMD of 0.1 95% CI: −0.2 to 0.2; p=0.872; 15 trials27 28 30 46 47 49–51 65–67 91–94; n=1780). At short-term, there was moderate evidence of no difference between telerehabilitation and control (SMD of 0.1 (95% CI: −0.3 to 0.4; p=0.795; three trials32 52 53; n=105) or other interventions (SMD of 0.3 (95% CI: −0.1 to 0.5; p=0.056; 30 trials26 33–35 37–39 41–45 55 56 58–60 62–64 67 69–71 87–90 95 96; n=2128) (figure 2).
Quality of life
For quality of life, overall effect analyses showed high-quality evidence that telerehabilitation was not different to other interventions at long-term (SMD: 0.2; 95% CI: −0.1 to 0.5; p=0.134; 10 trials27 29 30 47 50 51 65–67 94; n=1018) and moderate-quality evidence that telerehabilitation was not different to other interventions at short-term when compared with other intervention (SMD: 0.1; 95% CI: −0.2 to 0.5; p=0.522; 19 trials26 33 35 36 40 42 45 55 56 60–64 69–71 88 95; n=1902). The strength of the recommendation was low when telerehabilitation was compared with control at short-term (figure 2).
Effects of telerehabilitation on pain, physical function and quality of life for different subgroups of health conditions
Subgroup analyses using meta-regression to investigate the impact of clinical categories on the overall effect estimates were possible only when telerehabilitation was compared with other intervention because of small number of pooled trials (ie, <10 trials): outcome of pain at short-term; physical function at short-term and long-term; and quality of life at short-term. Qualitative analyses were conducted for the remained comparisons. Detailed subgroup analyses for all outcomes of interest are presented in figure 3.
Pain
When compared with other interventions at short-term, results of meta-regression showed impact of clinical categories on overall estimates (p<0.001). Qualitative subgroup analyses by clinical categories also suggested impact of subgroups on the overall estimates for pain. There was high-quality evidence of no difference between telerehabilitation and other intervention on pain at long-term for musculoskeletal conditions (SMD: −0.2; 95% CI: −0.4 to 0.1; p=0.114; four trials27 28 46 47; n=731) and moderate-quality evidence a small effect of telerehabilitation for postoperative orthopaedic conditions at short-term (SMD: −0.3; 95% CI: −0.7 to −0.1; p=0.026; five trials26 33 34 37 97; n=575). The strength of the recommendation was low and very low for all the other comparisons (figure 3).
Physical function
When compared with other interventions at short-term and long-term, results of meta-regression showed impact of clinical categories on overall estimates for physical function (p<0.001). High-quality evidence showed that telerehabilitation was not different to other interventions on physical function for pulmonary conditions at short-term and for musculoskeletal conditions at long-term. SMDs of 0.1 (95% CI: −0.1 to 0.4; p=0.204; four trials55 56 58 60; n=301) and −0.1 (95% CI: −0.2 to 0.4; p=0.540; five trials27 28 46 47 94; n=906) for pulmonary and musculoskeletal conditions, respectively. Besides, moderate-quality evidence showed a medium effect of telerehabilitation for oncology conditions at short-term (SMD: 0.6; 95% CI: 0.2 to 1.1; p=0.003; three trials69 90 96; n=191), a small effect of telerehabilitation for cardiovascular conditions at long-term (SMD: 0.4; 95% CI: 0.1 to 0.7; p=0.003; two trials51 92; n=223) and not different to other interventions at short-term for neurological (SMD: 0.2; 95% CI: −0.1 to 0.5; p=0.249; three trials38 39 95; n=174), cardiovascular conditions (SMD: 0.3; 95% CI: −0.2 to 0.7; p=0.237; eight trials35 36 62–64 70 71 88; n=570) and postoperative orthopaedic conditions (SMD: 0.2; 95% CI: −0.9 to 1.3; p=0.681; five trials26 33 34 37 89; n=577). As shown in figure 3, low to very-low quality evidence also suggested impact of different subgroups of health conditions on the estimates for physical function.
Quality of life
When compared with other interventions at short-term, meta-regression showed impact of clinical categories on overall estimates for quality of life (p<0.001). High-quality evidence showed that telerehabilitation was not different to other interventions on quality of life for musculoskeletal conditions at long-term (SMD: 0.3; 95% CI: −0.5 to 1.1; p=0.511; three trials27 47 94; n=400). Besides, moderate-quality evidence showed that telerehabilitation was not different to other interventions on quality of life at short-term for pulmonary, neurology and postoperative orthopaedic conditions. SMDs of 0.1 (95% CI: −0.2 to 0.3; p=0.624; three trials55 57 60; n=444), 0.1 (95% CI: −0.1 to 0.3; p=0.436; two trials40 95; n=321) and 0.9 (95% CI: −0.1 to 1.8; p=0.092; two trials26 33; n=385), respectively. Qualitative subgroup analyses suggested impact of subgroups on the remained comparisons for quality of life as well.
Sensitivity analysis
Meta-regression to investigate the impact of methodological issues was possible for few cases when telerehabilitation was compared with other interventions: pain at short-term; physical function at short- and long-term; and quality of life at short-term. Meta-regression showed impact of poor methods quality on overall estimates for pain at short-term, physical function at short-term and long-term and quality of life at short-term and long-term (p<0.001). Detailed qualitative sensitivity analyses by removing trials of poor methodological quality (<6 on the 0 to 10 PEDro scale) suggesting potential impact of poor methodological quality of included trials are presented in online supplemental material 5.
Supplemental material
Discussion
To our knowledge, this is the first systematic review with meta-analysis that investigated the effects of telerehabilitation on pain, physical function and quality of life in people with physical disabilities, when compared with control and other interventions. High-quality or moderate-quality evidence showed that telerehabilitation was not different to other interventions on pain at long-term, physical function at short-term and long-term and quality of life at short-term and long-term. Therefore, we are confident that the true effect lies close to the estimate of the effect and that telerehabilitation may be an alternative to treat people with physical disabilities. We have very little confidence in the effect estimate when telerehabilitation was compared with control.
In some included trials, telerehabilitation groups received more follow-up than the comparison groups, with more elaborate interventions preceded by conventional rehabilitation or periodic meetings during the intervention period. Hailey et al 98 pointed out in their review on telerehabilitation in routine care that, in most studies, telerehabilitation intervention was more elaborate than the comparator, with additional services and more frequent contacts between patients and professionals. Thus, the authors argue that the positive results found could be attributed to the use of more elaborate interventions. Moreover, some trials investigated interventions focussed not only on the exercise protocol, but incorporated other strategies such as a stimulus to increase physical activity, self-management, education and behavioural changes.25 27 28 31 43 46–48 59 73 Multicomponent interventions have been employed in different contexts to facilitate self-management of the disease and to involve the patient in their treatment.97 99 100 This type of intervention has shown better results when compared with single component interventions in chronic patients.100 Pietrzak et al 101 identified in their review that self-management programmes, education and exercises at a distance can be used successfully in patients with osteoarthritis, resulting in improvements in health status indicators, access to care and communication between patients and health professionals. To investigate whether different types and dosage of exercise by telerehabilitation would impact on estimates, we planned subgroup analyses; however, investigation was not possible because of the small number of included trials.
Overall, for the outcomes of physical function and quality of life, our results showed evidence of moderate and high quality for no difference between telerehabilitation and other interventions at short-term and long-term. Therefore, it is likely that telerehabilitation is equivalent to other forms of care. Possible mediating variables reinforced the beneficial effects that physical activity exerts on quality of life. Self-efficacy in older adults, for example, is a possible mediator of physical and psychological results associated with physical activity, by increasing the sense of control and satisfaction with the lives of these individuals.102 Specific studies of cardiac populations have shown similar results. Hwang et al 103 reported in their systematic review on the effects of telerehabilitation in patients with cardiopulmonary diseases that, in general, the telerehabilitation group significantly improved the quality of life of patients with cardiomyopathy. Chan et al 104 conducted a meta-analysis on exercise by telemonitoring and telerehabilitation compared with traditional cardiac and pulmonary rehabilitation. They concluded that, for patients with cardiac diseases, telerehabilitation provided similar benefits to usual care and without reports of adverse effects.
Efficacy
Finally, due to the low-quality evidence and the small number of trials comparing exercise protocols offered by telerehabilitation with control groups, it is still not possible to state the efficacy of telerehabilitation on pain, function and quality of life at short-term and long-term, for adults with physical disabilities. In general, evidence comparing telerehabilitation with control group without intervention was considered low or very low due to imprecision (grouping <400 participants), risk of bias (PEDro score <6) and/or inconsistency (I²>50%). Further high-quality trials comparing telerehabilitation with control to investigate efficacy on our population of interest are needed. It is also promising in postoperative orthopaedic, oncological, cardiovascular, pulmonary, neurological and musculoskeletal conditions.
The risk of bias of the trials was relatively low, with PEDro greater than 6 points out of 10 in more than half of the trials included in this review. This type of study, in recent years, has followed detailed guidelines and strict criteria for its publication. It is noteworthy that none of the trials reached the maximum score, which can be explained by the difficulty of blinding the participants and therapists, due to the characteristics of the interventions implemented by telerehabilitation. Two other limitations found in 50% of the included trials were the absence of concealed allocation and intention-to-treat analysis. These strategies have been recommended to preserve the integrity of randomisation and prevent bias caused by loss of participants.105 106 Without these, the benefits of randomisation may be lost.106
Limitations
This study has some limitations. A potential limitation was the heterogeneity across trials (eg, different clinical conditions and different telerehabilitation delivery modes pooled and risk of bias). To solve this potential limitation, we conducted clinical conditions subgroup and sensitivity analyses to explore their impact on the estimates using meta-regression when possible. Consistent findings showed that clinical categories and risk of bias impact on estimates. Subgroup analyses for telerehabilitation delivery mode was not possible due to small number of included trials. Another potential limitation was that our included trials assessed the same outcome of interest but measured it in different validated ways. In this context, we used SMDs to conduct meta-analysis in the current review. Although weighted mean differences are better for interpretation, SMDs are also allowed and recommended by the Cochrane77 to pool data from different measurements. Other sources of heterogeneity were also potential limitations, such as type and dosage of telerehabilitation. Exploration of their potential impact on the estimates was limited by the number of included trials and by missing data. To decrease these other potential limitations, we used random-effect models for pooling and did not consider trials reporting data not normally distributed in the quantitative analyses.77 Future trials with greater sample sizes and appropriate reported data should further investigate impact of types and dosage of exercise by telerehabilitation in our population of interest.
Conclusions
This systematic review with meta-analysis was developed to support decision-making related to public policies and health programmes. Policies based on scientific evidence have ensured that decisions are based on the best available scientific evidence. This systematic review indicates that exercise by telerehabilitation has at least similar effects on pain, physical function and quality of life when compared with other interventions. However, efficacy is still limited by the scarcity of trials and low certainty of the current evidence.
What is already known
Telerehabilitation has the capacity to provide equitable access to individuals who do not have access to services, whether for geographical, physical or economic reasons.
Telerehabilitation has the potential to improve quality of care, increase access to services and support health services.
What are the new findings
Exercise by telerehabilitation can lead to clinical results similar to other interventions in improvement of pain, physical function and quality of life at short-points and long-points.
Few studies compared exercise by telerehabilitation with control groups without any intervention, so it is still not possible to affirm the efficacy of telerehabilitation in reducing pain, function and quality of life in adults with physical disabilities.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JFD, VCO, PRTB, FCMSD, MCM, RNK, RAR and RFS contributed to planning, conduct and reporting of the work described in this article.
Funding This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. We are also thankful to the State of Minas Gerais Funding Agency FAPEMIG.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.