Article Text

Abstract
Objectives Coach-centred antidoping education is scarce. We tested the efficacy of a motivationally informed antidoping intervention for coaches, with their athletes’ willingness to dope as the primary outcome.
Methods We delivered a cluster randomised controlled trial in Australia, the UK and Greece. This study was a parallel group, two-condition, superiority trial. Participants were 130 coaches and 919 athletes. Coaches in the intervention group attended two workshops and received supplementary information to support them in adopting a motivationally supportive communication style when discussing doping-related issues with their athletes. Coaches in the control condition attended a standard antidoping workshop that provided up-to-date information on antidoping issues yet excluded any motivation-related content. Assessments of willingness to dope (primary outcome) and other secondary outcomes were taken at baseline, postintervention (3 months) and at a 2-month follow up.
Results Compared with athletes in the control group, athletes in the intervention group reported greater reductions in willingness to take prohibited substances (effect size g=0.17) and psychological need frustration (g=0.23) at postintervention, and greater increases in antidoping knowledge (g=0.27) at follow-up. Coaches in the intervention group reported at postintervention greater increases in efficacy to create an antidoping culture (g=0.40) and in perceived effectiveness of need supporting behaviours (g=0.45) to deal with doping-related situations. They also reported greater decreases in doping attitudes (g=0.24) and perceived effectiveness of need thwarting behaviours (g=0.35).
Conclusions Antidoping education programmes should consider incorporating principles of motivation, as these could be beneficial to coaches and their athletes. We offer suggestions to strengthen these programmes, as most of the effects we observed were not sustained at follow-up.
Trial registration number This trial has been registered with the Australian New Zealand Clinical Trials Registry (https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=371465&isReview=true).
- doping
- education
- intervention
- randomised controlled trial
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
A meta-analysis1 of psychosocial predictors of doping use in physical activity revealed two significant problems in the antidoping literature: the scarcity of field-based intervention studies, and the overemphasis on athlete variables (eg, attitudes, beliefs and perfectionism) as predictors of doping intentions and use. A 2018 editorial2 also highlighted the need to address individual, social and environmental factors in antidoping policy and practice. Coaches represent a significant social factor in shaping athletes’ cognitions, emotions and behaviour; several coach characteristics (eg, doping confrontation efficacy) have been linked to athletes’ propensity to engage in doping or their susceptibility to inadvertent doping.3 4
Can changing coaches’ communication style facilitate changes in athletes’ antidoping-related attitudes and behaviour? Self-determination theory (SDT)5 suggests that the communication styles adopted by people in positions of authority vary in the degree to which they support or undermine the psychological needs for autonomy, competence and relatedness (and subsequent motivation, well-being and behaviour) of those they instruct. In a prospective survey study6 of 166 athletes, perceptions of a need-supportive coach communication style predicted satisfaction of athletes’ basic psychological needs, positive moral attitudes, lower intention to dope and less self-reported doping use.
To date, there are no interventions that have examined how targeting coaches’ communication style can predict changes in doping-related cognitions and behaviours in athletes, and how coaches can benefit from such an intervention. Coaches often lack confidence and knowledge to engage in antidoping discussions with their athletes, and are often reluctant to participate in antidoping education programmes.7–9 Therefore, we aimed to test a large-scale antidoping education intervention for coaches in three countries using a cluster randomised controlled trial (RCT) design. Our antidoping education programme incorporated principles of motivational theory to help coaches (a) create a need supportive motivational atmosphere within their team (hence, reducing the willingness to use prohibited substances) and (b) use need supportive communication when promoting antidoping behaviour (eg, testing, checking medication) with their athletes. The comparator was a standard antidoping information programme that provided up-to-date information on various antidoping issues but excluded any motivation-related content. We hypothesised that the intervention group of coaches (and indirectly their athletes) would benefit more from the intervention than the control group. No a priori country differences were identified. All hypotheses and outcome measures (and a justification for their selection) were preregistered in our protocol.10
Method
Study design
This study was a cluster RCT, delivered in Australia, the UK and Greece. We implemented and tested a parallel group, two-condition, superiority trial.
Settings and participants
Coach and athlete demographic characteristics are presented in table 1. The intervention targeted sport coaches from various popular sports in each country; no direct intervention was provided to their athletes. We recruited coaches (one per team) who coached athletes aged 14 years or older, trained at least once a week and competed (at any level) on a regular basis. We did not have any eligibility criteria based on coach demographics. We specified in our protocol10 an intraclass correlation coefficient of 0.05 (the 0.005 estimate was an overlooked typing error) and a small effect size (δ=0.22) for the primary outcome, and estimated an average of 10 athletes per coach. Using Optimal Design Software11 for clustered RCTs with treatment at level 2 and primary outcome at level 1, our power with 106 coaches at follow-up was 0.84 (power was 0.92 at baseline with 130 coaches and 0.89 at follow-up with 122 coaches). Recruitment occurred over a 12-month period via a variety of means (eg, face-to-face, emails and social media). Assessments were taken at club venues at baseline, end of intervention (12 weeks) and 2 months later (follow-up). No unintended consequences or harms were reported.
Athlete and coach baseline characteristics
Randomisation and blinding
Sport clubs within each country were randomly assigned to either condition via computer software,12 with a 1:1 allocation using permuted undisclosed blocks of random sizes. The randomisation was carried out by a research team member who was not involved in participant enrolment. Research assistants who collected data were blinded to condition allocation throughout the study, but due to the nature of the intervention coaches could not be blinded. Hence, multiple coaches from the same club were assigned to the same condition.
Interventions
Standard antidoping education
Coaches received a ‘standard’ antidoping small-group workshop with no motivational content. The workshop covered important issues in doping prevention,13 such as antidoping rule violations, list of prohibited substances, therapeutic use exemptions, testing procedures and how to check the contents of supplements and medications. Several related resources were given to coaches to reinforce learnings from the workshop. The coaches were invited to receive the intervention workshops after all assessments were completed.
Motivationally enriched antidoping education
Coaches received the same antidoping information as in the standard condition, yet were trained to deliver this information using need supportive communication styles. Coaches participated in two small group workshops. Workshop 1 was delivered in the first week and introduced need supportive communication. Workshop 2 was delivered in week 5 and aimed to upskill coaches in how to apply need supportive communication to discuss doping-related issues with their athletes. During 12 weeks of the intervention, coaches were provided with material (eg, planning sheets; see protocol paper10 for full details) to help them apply the skills taught in the workshops. Each country had several facilitators who delivered the workshops in one or both conditions. Each facilitator was trained to deliver the content of each workshop in a standardised way via a checklist.
Outcomes
We collected self-reported demographics from coaches and athletes at baseline. All other variables were assessed on 7-point rating scales, unless specified otherwise later. The primary outcome was athletes’ willingness to take prohibited substances. Secondary outcomes were athletes’ moral disengagement in doping, attitudes towards doping, efficacy to resist doping-related temptations, engagement with six behaviours (eg, checking medication on GlobalDRO) over the past 4 weeks to prevent inadvertent doping (yes/no), knowledge about six antidoping testing procedures (true/false/unsure), perceived need supportive and need thwarting coach behaviours and satisfaction and frustration of psychological needs. We also assessed (as secondary outcomes) coach reports of moral disengagement in doping, attitudes towards doping, efficacy to discuss doping-related issues with athletes, efficacy to create an antidoping team culture (0%=no confidence to 100%=complete confidence), knowledge about six antidoping testing procedures (true/false/unsure), encouragement of athletes over the past 4 weeks to engage in six behaviours to prevent inadvertent doping (yes/no) and perceived effectiveness of need supportive and need thwarting coach style in dealing with doping-related situations. The scales for all measures are reported in our protocol.10
Statistical analysis
We tested changes in study outcomes within a multilevel framework using Mplus V.8.2.14 To facilitate model convergence, we used a Bayesian estimator with non-informative priors to ensure that the data drove the characterisation of the posterior distribution.15 The effects of the intervention were tested using all randomised participants who were retained in the analysis irrespective of whether they dropped out or not (ie, all available cases). The Gibbs sampler was used to treat missing observations as unknown values to be estimated using the algorithm under the missing at random assumption.15 Our approach follows recommendations16 for treatment of missing data in RCTs which suggest that statistical analyses should include all observed data that are valid under a plausible assumption about the missing data. The results of a sensitivity analysis included responses only from those individuals who completed all assessment periods (ie, list-wise deletion). Simulation data17 support the superiority of modern approaches like Bayesian estimation for handling missing data when compared with traditional approaches such as list-wise deletion. Hence, our interpretations are based on the analyses that included all available cases.
Athlete data included three levels in the analysis, with repeated measures (level 1) nested within athletes (level 2) nested within coaches (level 3). Analysis of two random slopes of time on the outcome variable at level 1 provides an understanding of athletes’ increase or decrease in outcomes from pre–postintervention (slope 1) and postintervention to follow-up (slope 2). At level 2, experimental condition (0=control, 1=intervention) and country effects were entered as predictors of the random slopes. The effect of the experimental condition on the random slopes provides an indication of differences between the intervention groups at postintervention and follow-up (ie, time × experimental condition interactions). We created two dummy variables to represent the Greek (GRC=0.67, UK/AUS=−0.33) or British (UK=0.67, GRC/AUS=−0.33) athletes as the reference group. With this effect coding, the dummy coefficient represents the difference between the Greek sample (or the British sample) from the average of all three countries on the dependent variable.18 We controlled for athlete demographics (gender [0=female, 1=male], age, hours per week spent training and number of years with their current coach) at level 2. Adjusted analysis takes into account expected differences in prognostic factors between groups that may influence the outcomes. Coach data included two levels in the analysis, with repeated measures (level 1) nested within coaches (level 2). At level 2, demographic variables (age, gender [0=female, 1=male]), previous doping education (0=no, 1=yes) and number of years coaching), experimental condition (0=control, 1=intervention) and country effects were entered as predictors of the random slopes of time on the outcome variable. As per CONSORT guidelines,19 we did not test for baseline group differences. Inferences regarding the meaningfulness of effects were based on whether or not credibility intervals (CIs) incorporated zero.
Public and patient involvement
Prior to the trial, experienced educators from national antidoping agencies (eg, Head of Education and antidoping educators working on behalf of a national antidoping agency), sport governing bodies and coaches provided feedback on the intervention material (following which we made slight changes in wording and content structure) and study design, and helped with recruitment and dissemination. Coaches were also interviewed at the end of the project about the impact of the programme on them and their athletes. None of these individuals were involved in the selection of outcome measures.
Deviations from registered protocol
None.
Results
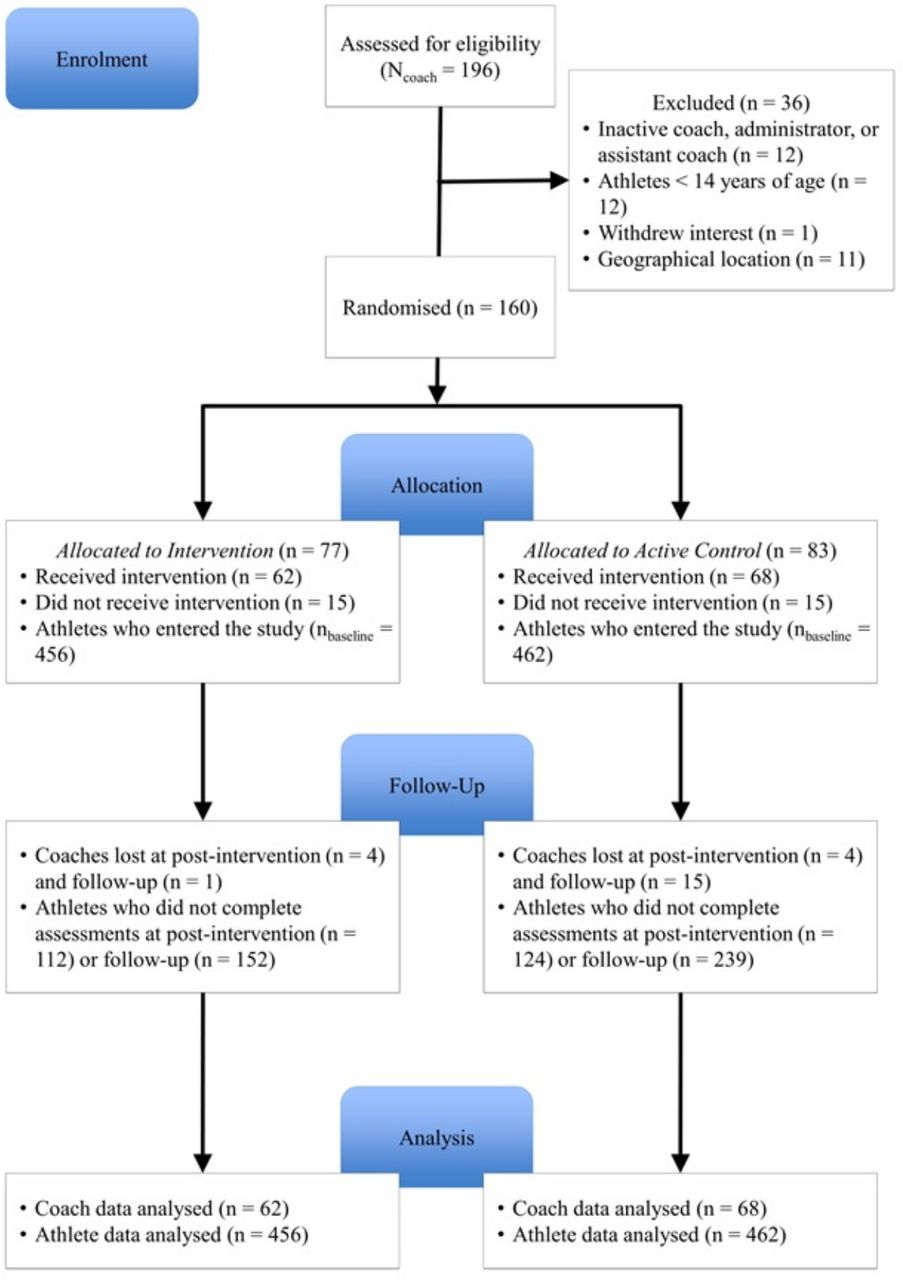
The flow of participants through the experimental procedures is provided in figure 1. Unadjusted descriptive statistics, omega coefficients for internal reliability and sample sizes for athlete and coach outcomes at baseline, postintervention and follow-up are presented in tables 2 and 3, respectively. Intervention effects for athlete and coach reported data are shown in tables 4 and 5, respectively, and statistically significant interactions are presented in online supplemental figures S1 and S2. Rules of thumb for effect size Hedge’s g are 0.20 (small), 0.50 (medium) and 0.8 (large). Study retention rates were satisfactory at the end of the 12-week programme (~74% for athletes and ~94% for coaches) and at 2-month follow-up (~57% for athletes and ~82% for coaches).
Supplemental material

{kind=link}
CONSORT flow diagram.
Unadjusted means (SD) of athlete reported outcomes
Unadjusted means (SD) of coach reported outcomes
Adjusted differences between experimental groups on athlete-reported outcomes for all case analysis and sensitivity analyses
Supplemental material
Adjusted differences between experimental groups on coach-reported outcomes for all case analysis and sensitivity analyses
Primary outcome
Compared with athletes in the control group, athletes coached by intervention group coaches reported a greater decrease in willingness to take prohibited substances at postintervention (mean difference (MD)=−0.16, 95% CI=−0.30, −0.03), but not at follow-up.
Secondary outcomes
Compared with athletes in the control group, athletes coached by intervention group coaches reported a greater decrease in need frustration at postintervention (MD=−0.24, 95% CI=−0.41, −0.06), and a greater increase in antidoping knowledge at follow-up (MD=0.42, 95% CI=0.08, 0.78).
Coaches in the intervention group reported greater increases in efficacy to create an antidoping culture (MD=4.46, 95% CI=0.93, 8.01) and in perceived effectiveness of need support behaviours to deal with doping-related situations (MD=0.35, 95% CI=0.06, 0.64), and greater decreases in doping attitudes (MD=−0.10, 95% CI=−0.20, −0.002) and perceived effectiveness of need thwarting behaviours to deal with doping-related situations (MD=−0.40, 95% CI=−0.77, −0.03) at postintervention. At follow-up, coaches in the intervention group reported greater decreases in their encouragement of athletes to engage in six behaviours to prevent inadvertent doping (MD=−0.99, 95% CI=−1.85, −0.14) and greater increases in perceived effectiveness of need thwarting behaviours (MD=0.47, 95% CI=0.04, 0.90). Country differences were minor and inconsistent (see online supplemental material).
Discussion
Athlete outcomes
We found a significant time × group effect at the end of the intervention for our primary outcome. There were steeper decreases in willingness to dope for athletes whose coaches received the need supportive communication training (g=0.17). Previous research20 has suggested that athletes may be willing to dope when they find themselves in a risk-conducive situation (eg, under distress), even if they have no prior intention to dope. Hence, equipping coaches with communication skills to deal with such situations in ways that do not undermine athletes’ psychological needs could be helpful in terms of decreasing athletes’ willingness to dope. Relatedly, athletes in the intervention group reported lower psychological need frustration at the end of intervention, compared with athletes in the control group. This finding is important because when athletes’ basic psychological needs are undermined, they report maladaptive outcomes, such as feelings of exhaustion and doping intentions/doping use.6 21
Contrary to our hypotheses, we did not find athletes in the intervention group to perceive their coaches as being more need supportive and less need thwarting from preintervention to postintervention, compared with athletes in the control group. Need supportive communication interventions in sport usually attract individuals who are more need supportive, hence possibly why in both conditions perceptions of coaches’ need support were high.22 Nevertheless, there are two results in support of our programme. The first finding is the greater reduction in athletes’ perception of their needs being frustrated (which has been directly linked to reductions in perceptions of a need thwarting coaching style23). The second finding is the significant group × time effects in favour of the intervention with regard to coaches’ perceived effectiveness of need support and need thwarting communication styles for discussing with their athletes doping-related situations. Specifically, at the end of the intervention, coaches in the intervention group reported greater increases in the effectiveness of need supporting strategies (eg, ‘demonstrating affection and care’), and greater decreases in the effectiveness of need thwarting strategies (eg, ‘impose rules with no explanations’), compared with coaches in the control group.
We also found that athletes in the intervention group reported greater increases in antidoping knowledge at follow-up, compared with athletes in the control group. Given that no aspects of the intervention were directly delivered to athletes, this finding is encouraging. It suggests that coaches in the intervention arm engaged in discussions with their athletes about doping in a more meaningful way than coaches in the control arm (who were given the same factual information but no training in terms of communication styles), which translated into improved knowledge retention for athletes. However, we found no group × time interactions for behaviours that protect athletes from inadvertent doping, indicating that our training did not help athletes in the intervention group to increase the number of risk-reducing behaviours to prevent unintentional doping. This finding could be partly because some of the items we used were inapplicable to our athletes (ie, they did not take medication or did not have access to sport science or medical professionals to consult). We also found no significant time × group interactions in athletes’ reports of moral disengagement in doping, doping attitudes and doping efficacy. Changes in these variables might require an intervention focus on theoretically more closely aligned antecedent variables, such as moral identity,24 beliefs and social norms,25 and not on coach communication styles.
Coach outcomes
Our intervention was not powered to detect changes in coach outcomes. Nevertheless, given the scarcity of research on how antidoping programmes can benefit coaches, and the reluctance of coaches to engage in such programmes,9 we consider it important to document the preliminary effects of our intervention with respect to changing coach outcomes. We found significant group × time effects at postintervention, in favour of the coaches in the intervention group, in terms of decreasing doping attitudes and perceptions of effectiveness of a need thwarting style and increasing efficacy to create an antidoping team culture and perceptions of how effective a need supportive style is in dealing with doping-related situations. There were no group differences in efficacy to discuss doping issues, antidoping knowledge and encouragement of athletes to engage in behaviours to prevent inadvertent doping. This finding suggests that, as intended, both groups received comparable education in terms of factual antidoping information. Two surprising results were found at follow-up in favour of the control group in terms of inadvertent doping prevention and perceived effectiveness of need thwarting. However, all findings at follow-up should be interpreted with caution given the small sample of coaches and the greater dropout in the control group at that time point.
How effective was the intervention?
The intervention had positive effects on the primary outcome and several secondary outcomes at the athlete and coach levels. However, such effects were small to moderate and not maintained following the end of the intervention, indicating the need for booster sessions that reinforce and build on intervention messages.26 An overview22 of need supportive communication interventions in sport has identified a number of barriers that limit the effectiveness of SDT training, such as perceptions that time and practical constraints limit opportunities to be need supportive, and beliefs that such training is idealistic, impractical and in contrast to cultural norms regarding coach authority. Such barriers could have prevented coaches from fully engaging with and applying our communications training. It is also possible that focusing on coaches only was not sufficient to produce lasting changes. Future deliveries should consider including other support personnel and athletes in the training2 to ascertain whether our programme can result in improved outcomes, particularly at follow-up. Also, focusing on additional variables, such as habit formation,27 might strengthen the programme’s long-term changes.
Strengths and Limitations
This trial is the largest published study of an antidoping intervention programme delivered to sport coaches. It addresses identified gaps in antidoping practice,1 is consistent with the 2015 WADA Code recommendations for enhanced education of athlete support personnel, uses a novel and theory-informed approach to antidoping education (ie, coach motivational training), a rigorous design (cluster RCT) and statistical analysis, has a large sample of coaches and athletes across three countries and reports longitudinal changes in coach and athlete outcomes with some objective data (ie, antidoping knowledge). A limitation of our work is the attrition rate in the athletes (particularly in the control group), and that the two groups received unequal attention in terms of amount of training. However, the antidoping education offered to the control group reflected current standard antidoping practice. A further limitation was that the types of sports in the intervention and control conditions were not identical.
Key messages
What are the findings?
The 12-week intervention had positive effects on indices of motivation (athletes’ reports of psychological need frustration, coaches’ perceptions of effectiveness of need supportive and need thwarting coaching styles), athletes’ willingness to dope and knowledge about antidoping.
The two groups of coaches did not differ in terms of antidoping knowledge or efficacy to apply such knowledge, which is unsurprising as both groups received comparable information on antidoping issues.
The intervention effects dissipated after the end of the intervention.
How might it impact on clinical practice in the future?
Future antidoping education programmes should consider training coaches in need supportive communication style, as such training (with potential booster sessions) could be beneficial to coaches and their athletes.
References
Footnotes
Twitter @NikosNtoumanis, @susanbackhouse, @DanielGucciardi
Contributors NN, DFG, SHB, VB, EQ and LP conceived the project and obtained the project funding. EQ, NN, LW, LP and SHB contributed to the development of the intervention materials. GP, SK and VB translated all material in Greek. BJS, LW, HRS, GP and SK managed the project on a daily basis in the three countries and coordinated data collection. NN and DFG wrote the first draft of the manuscript. All authors contributed to the refinement of the manuscript and approved the final version.
Funding This project was supported by funding from the International Olympic Committee. The International Olympic Committee had no authority in the study design, collection, management, analysis or interpretation of the data.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethics Committees of all participating universities and all participants signed a consent form.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Deidentified participant SPSS data file and Mplus code for all analyses conducted are available from Nikos Ntoumanis (nikos.ntoumanis@curtin.edu.au) or Daniel Gucciardi (d.gucciardi@curtin.edu.au). Interested parties need to explain why and how they are planning to reuse the data.