Article Text

Abstract
Background Knee MRI is increasingly used to inform clinical management. Features associated with osteoarthritis are often present in asymptomatic uninjured knees; however, the estimated prevalence varies substantially between studies. We performed a systematic review with meta-analysis to provide summary estimates of the prevalence of MRI features of osteoarthritis in asymptomatic uninjured knees.
Methods We searched six electronic databases for studies reporting MRI osteoarthritis feature prevalence (ie, cartilage defects, meniscal tears, bone marrow lesions and osteophytes) in asymptomatic uninjured knees. Summary estimates were calculated using random-effects meta-analysis (and stratified by mean age: <40 vs ≥40 years). Meta-regression explored heterogeneity.
Results We included 63 studies (5397 knees of 4751 adults). The overall pooled prevalence of cartilage defects was 24% (95% CI 15% to 34%) and meniscal tears was 10% (7% to 13%), with significantly higher prevalence with age: cartilage defect <40 years 11% (6%to 17%) and ≥40 years 43% (29% to 57%); meniscal tear <40 years 4% (2% to 7%) and ≥40 years 19% (13% to 26%). The overall pooled estimate of bone marrow lesions and osteophytes was 18% (12% to 24%) and 25% (14% to 38%), respectively, with prevalence of osteophytes (but not bone marrow lesions) increasing with age. Significant associations were found between prevalence estimates and MRI sequences used, physical activity, radiographic osteoarthritis and risk of bias.
Conclusions Summary estimates of MRI osteoarthritis feature prevalence among asymptomatic uninjured knees were 4%–14% in adults aged <40 years to 19%–43% in adults ≥40 years. These imaging findings should be interpreted in the context of clinical presentations and considered in clinical decision-making.
- knee
- mri
- osteoarthritis
- cartilage
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
MRI is the most reliable non-invasive diagnostic technique to assess internal derangement of the knee joint. Increasing MRI availability has resulted in a rapid rise in its utilisation to help inform clinical management of patients with knee symptoms.1 2 Over $14 billion is spent on diagnostic imaging in the USA annually,3 yet the overall clinical benefit of the current use of knee MRI is uncertain.4 5 Findings such as meniscal tears, cartilage defects, bone marrow lesions (BMLs), osteophytes and other features suggestive of knee osteoarthritis (OA) are often interpreted as causes of pain and symptoms, triggering medical and surgical interventions.6 7 However, the relationship between MRI features of OA and knee pain is imprecise.8
In patients with knee OA, there is moderate evidence that MRI-assessed BMLs and effusion/synovitis are associated with knee pain, but conflicting or limited evidence for other MRI findings.8 Features associated with OA have also been observed on MRI in asymptomatic uninjured knees,9–11 suggesting that MRI-assessed OA features may not necessarily be the source of pain in symptomatic patients. However, estimates of the prevalence of MRI features of OA in asymptomatic uninjured knees vary across studies, from 0% to 75%.9 10 Given the large number of adults undergoing MRI to investigate the cause of knee symptoms, a reliable estimate of the prevalence of MRI features of OA in asymptomatic uninjured knees is important to inform efforts to diagnose and treat knee symptoms across the lifespan. Therefore, the aim of this systematic review and meta-analysis was to determine the prevalence of, and factors contributing to, MRI features of OA in asymptomatic uninjured knees.
Methods
Search strategy and selection criteria
This systematic review conforms to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines and is registered with PROSPERO (CRD42016053969). Study investigators searched for studies reporting the prevalence of MRI features of knee OA in asymptomatic adult knees (ie, mean age ≥18 years with no knee symptoms during any activity) with no history of injury or surgery in EMBASE, Medline, CINAHL, SPORTDiscus, Web of Science and Scopus from inception to the day of the search on 24 October 2017. The searches combined terms related to knee, asymptomatic, MRI, and pathology, without language restriction and adjusted according to individual database specifications (online appendix eMethods 1).
Supplementary file 1
Primary outcomes were individual MRI features assessed semiquantitatively and included in the definition of MRI-defined knee OA12: (i) cartilage defects, defined as partial-thickness or full-thickness cartilage lesions; (ii) meniscal tears, defined as high signal extending to an articular surface; (iii) BMLs, defined as areas of ill-delineated signal within trabecular bone (hypointense on T1-weighted images, hyperintense on T2-weighted fat-suppressed images); and (iv) osteophytes, defined as the presence of osteocartilagenous protrusions at articular margins. Secondary outcomes were other MRI features previously associated with knee OA (defined in detail in the online appendix eMethods 2): effusion-synovitis, subchondral cysts, ligament tears, subchondral sclerosis/attrition and infrapatellar fat pad synovitis/oedema. Two authors (AGC, HFH) independently assessed all titles and abstracts of identified reports for eligibility. Reference lists of all publications considered for inclusion were hand-searched recursively until no additional eligible publications were identified. When eligibility could not be confirmed from title and abstract, full texts were reviewed and study investigators contacted as required. If authors were able to provide data from the subset of asymptomatic participants without prior index knee injury or surgery, these were included, otherwise the article was excluded. Only full-text published articles were eligible. No publication was excluded based on language or study design. Detailed eligibility criteria are described in the online appendix eMethods 3.
Data extraction
The following information was independently extracted from the included studies by two investigators (AGC, JJS): number of participants/knees, participant characteristics (eg, age, sex, body mass index (BMI), sporting/physical activity level), MRI sequences, outcome definition (ie, specific diagnostic criteria) and reported prevalence of whole knee, as well as compartment-specific (ie, tibiofemoral and patellofemoral), abnormalities. The publication with the most participants (or most OA features assessed) was used when several publications used the same population.
Risk of bias assessment
Two reviewers (AGC, BEØ) independently assessed risk of bias using a 13-item checklist developed specifically for this review assessing quality of reporting, sample representativeness and size, comparability between respondents and non-respondents, distribution of confounders and ascertainment of MRI features of OA (online appendix eMethods 4). As per the Cochrane Handbook for Systematic Reviews recommendations, we customised specific items from the Downs and Black checklist for randomised and non-randomised studies,13 and a population-based prevalence study checklist.14 Items related to randomisation, intervention and others not relevant for the current review were excluded. Items were scored as adequate, inadequate or unable to determine. Discrepancies were resolved by discussion.
Data synthesis and analysis
Prevalence estimates of the primary outcomes at a per-knee level were calculated by pooling the study-specific estimates using random-effects proportion meta-analysis that accounted for between-study heterogeneity (Stata V.14.2 metaprop command).15 Freeman-Tukey arcsine transformation was used to normalise variance. Binomial proportion 95% CIs for individual studies were calculated around study-specific and pooled prevalences based on the score-test statistic.16 Due to the incidence of degenerative changes generally increasing substantially after 40 years of age,17 prevalence estimates of the primary outcomes were calculated separately for studies with a mean age of <40 years and for those with a mean age ≥40 years. Secondary outcomes were often inconsistently defined and thus, descriptively synthesised. Between-study heterogeneity was evaluated for each primary outcome using standard Q-tests and the I2 statistic (ie, the percentage of variability in prevalence estimates that is due to heterogeneity rather than chance, 0%=no inconsistency, 100%=maximal inconsistency).18 We further explored between-study heterogeneity by comparing results from studies grouped according to several study level characteristics (detailed in the online appendix eMethods 3) using stratified meta-analysis and meta-regression. Study level characteristics assessed were age, sex, MRI sequences employed (summarised in the online appendix eTable 1), participation in weight-bearing sports, radiographic knee OA, sample size and overall risk of bias. The prevalence estimates of primary compartment-specific outcomes (ie, tibiofemoral and patellofemoral cartilage defects, BMLs, osteophytes; medial and lateral meniscal tears) were pooled wherever reported and differences between compartments assessed with a two-proportion z-test. Publication bias of the primary outcomes secondary to small study effects was assessed using funnel plots and the Egger test when meta-analysis included ≥10 studies. We also conducted sensitivity analyses excluding studies reporting the prevalence of primary outcomes from both knees of each participant to account for potential within-person correlations. All analyses were performed using Stata V.14.2 with a significance threshold of p<0.05.
Results
Study characteristics
Forty-six cross-sectional9 11 19–62 and 17 longitudinal studies10 63–78 involving a total of 4751 individuals (5397 knees) were included in this review (figure 1, table 1). Thirty-two took place in North America, 11 in Australia, 12 in Europe, 7 in Asia and 2 in Africa. The median number of participants and knees per study was 27 (range, 4–836) and 40 (range, 4–836), respectively. The diagnostic criteria used by the studies are summarised in the online appendix eTable 1. Out of 13 possible points on the risk of bias scoring criteria, 5 studies scored 0–4 points, 26 scored 5–7 points, 25 scored 8–10 points and 7 scored 11–13 points (details in the online appendix eTable 1, efigure 1).

Flow diagram for identifying studies.
Summary of included studies investigating the prevalence of MRI assessed knee OA features prevalence in asymptomatic uninjured populations
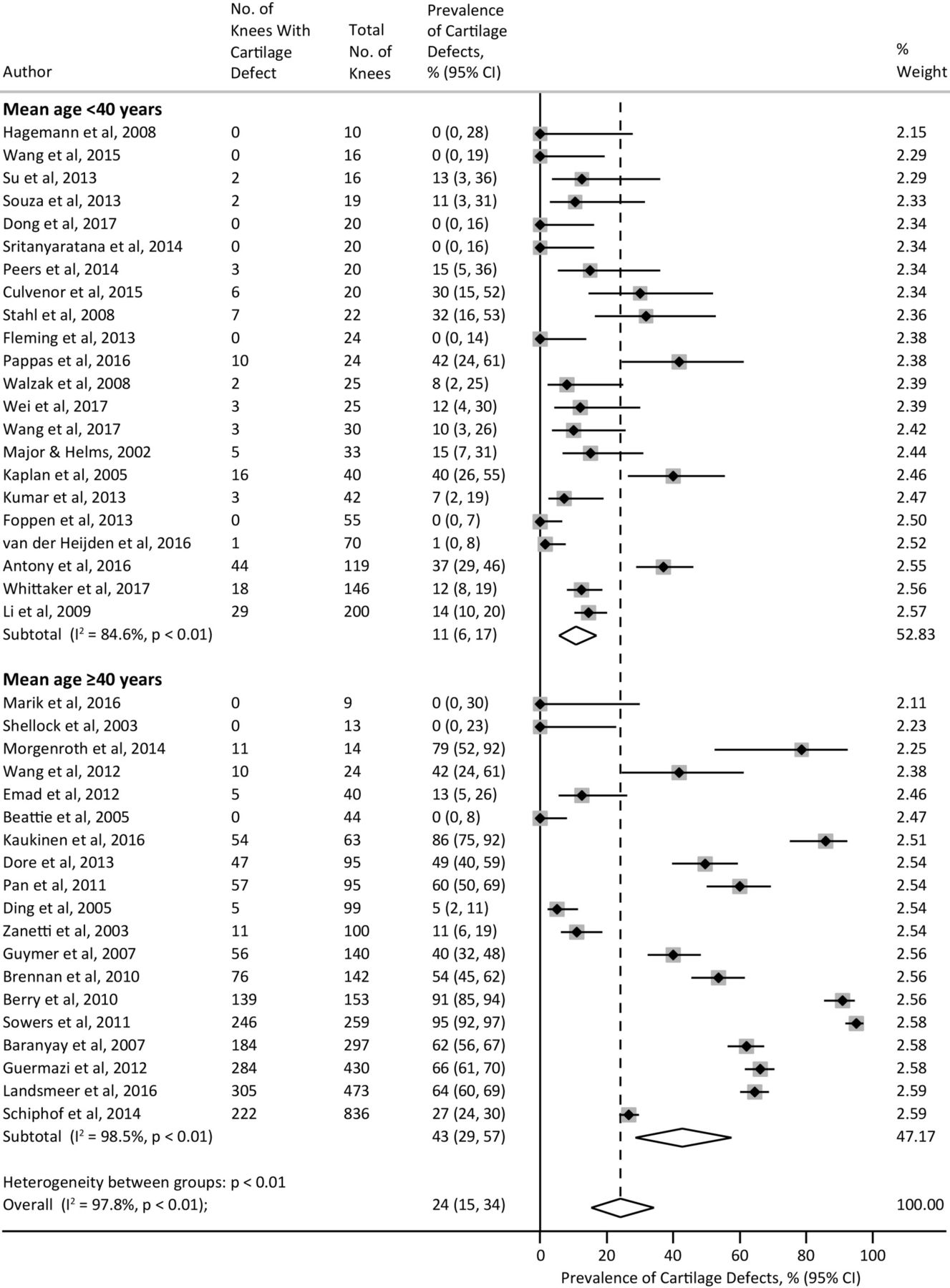
Prevalence of articular cartilage defects
Forty-two studies (4322 knees from 3446 participants) reported the prevalence of cartilage defects with an overall pooled prevalence estimate of 24% (95% CI 15% to 34%; I2=97.8%). Studies with a mean age <40 years and ≥40 years had a pooled prevalence of 11% (6% to 17%) and 43% (29% to 57%), respectively, with significant evidence of between-study heterogeneity (I2=84.6% and 98.5%, respectively) (figure 2). The prevalence of cartilage defects significantly increased with age (slope=14.4% increase per 10 years; 95% CI 9.0% to 19.9%, p<0.001) (online appendix efigure 2) and a higher proportion of women (slope=4.3% increase per 10% increase in proportion of women; 95% CI 1.3% to 7.3%, p=0.006). Heterogeneity was not accounted for by other factors evaluated except: (i) risk of bias score in studies with a mean age <40 years, where a lower risk of bias resulted in a higher prevalence (p=0.03; online appendix efigure 3; and (ii) sample size in studies with a mean age ≥40 years, where a sample of ≥50 knees resulted in a significantly higher prevalence (55% (95% CI 39% to 71%)) than samples of <50 knees (15% (0% to 42%)) (p=0.014) (online appendix eTable 3).

Meta-analysis of the prevalence of cartilage defects.
Prevalence of meniscal tears
Forty-four studies (3761 knees from 2817 participants) reported prevalence of meniscal tears with an overall pooled prevalence estimate of 10% (95% CI 7% to 13%; I2=87.2%). Studies with a mean age <40 years and ≥40 years had a pooled prevalence of 4% (2% to 7%) and 19% (13% to 26%), respectively, with significant evidence of between-study heterogeneity (I2=60.2% and 92.9%, respectively) (figure 3). The prevalence of meniscal tears significantly increased with age (slope=3.2% increase per-10 years, 95% CI 0.2% to 6.1%, p=0.036) (online appendix eFigure 2) and a higher proportion of women (slope=0.2% increase per 10% increase in proportion of females; 95% CI −1.4% to 1.8%, p=0.797). Prevalence of meniscal tears did not differ by any other study level characteristic except MRI sequences used in studies with a mean age <40 years, where use of optimal MRI sequences resulted in a significantly lower pooled prevalence (3% (0% to 7%)) than studies using suboptimal MRI sequences (7% (4% to 10%)) (p=0.034) (online appendix eTable 3).
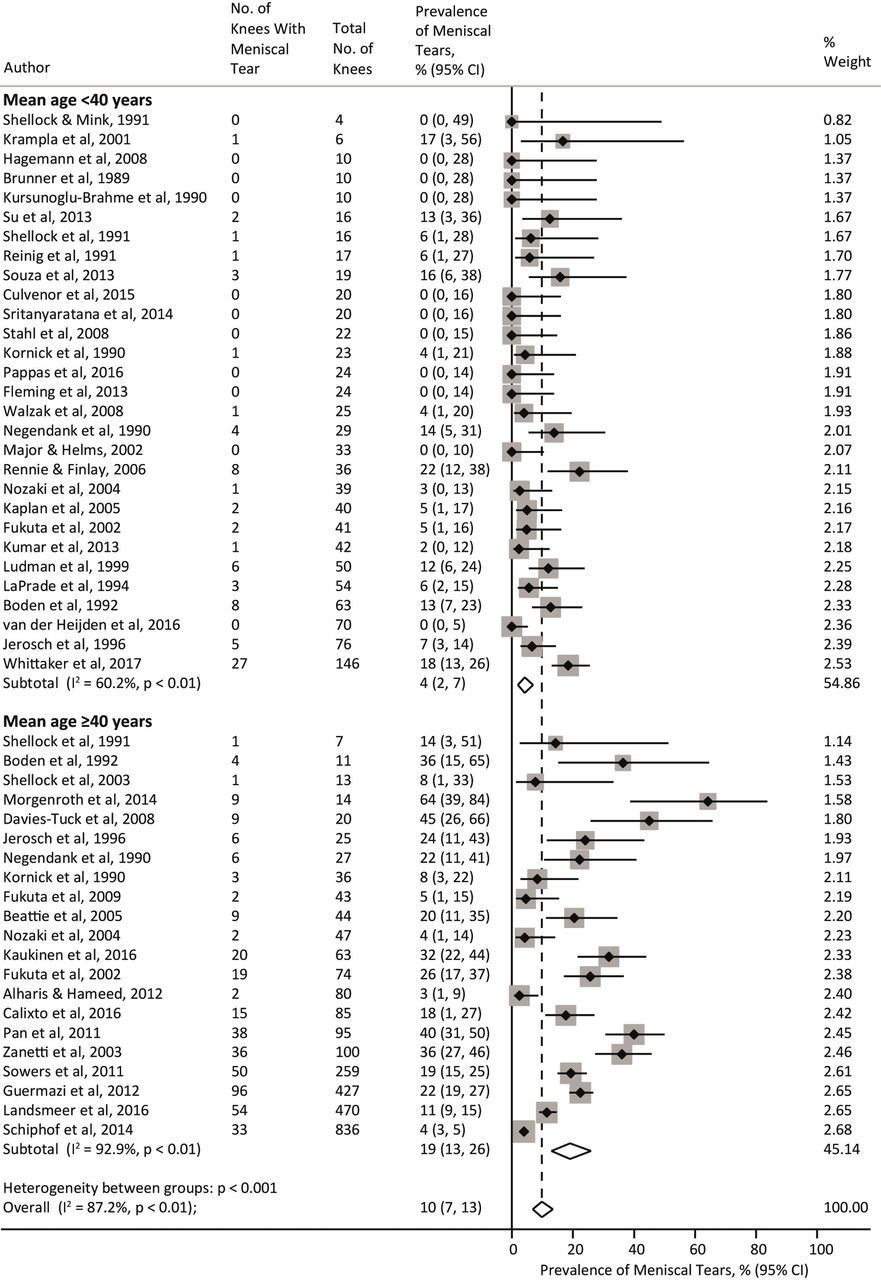
Meta-analysis of the prevalence of meniscal tears.
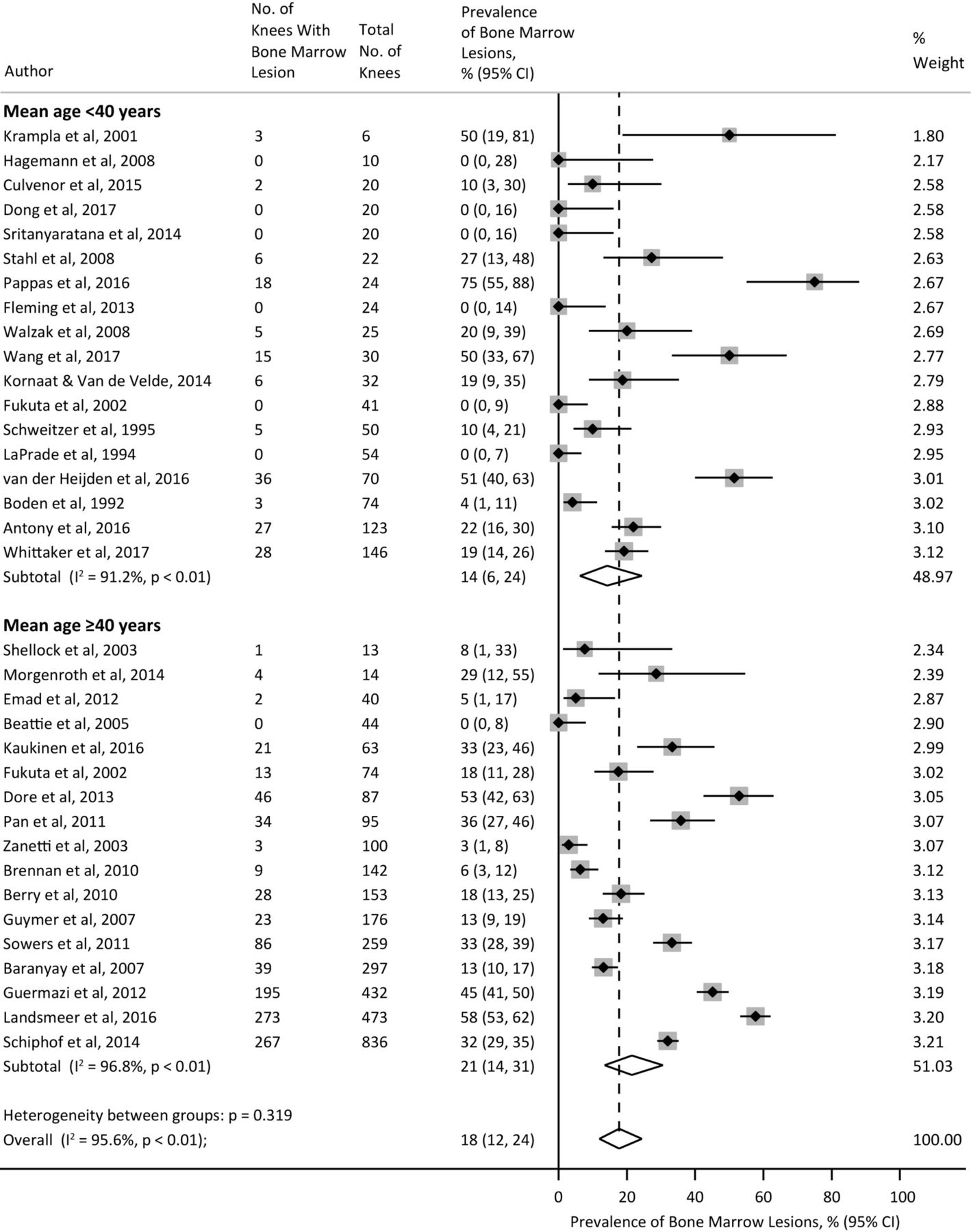
Prevalence of BMLs
Thirty-four studies (4089 knees from 3255 participants) reported BML prevalence with an overall pooled prevalence estimate of 18% (95%CI 12% to 24%; I2=95.6%). Studies with mean age <40 years and ≥40 years had a pooled prevalence of 14% (6% to 24%) and 21% (14% to 31%), respectively, with significant evidence of between-study heterogeneity (I2=91.2% and 96.8%, respectively) (figure 4). While BML prevalence was not associated with age (slope=4.3% increase per 10 years; 95% CI −0.4% to 9.1%, p=0.076) (online appendix eFigure 2) or percentage of women (slope=1.2% increase per 10% increase in proportion of women; 95% CI −1.5% to 3.9%, p=0.370), the large heterogeneity in those aged <40 years was partly explained by participation in weight-bearing sports. Studies of athletes playing weight-bearing sports resulted in a pooled estimate of 30% (17% to 45%) compared with general population studies of 3% (0% to 11%) (p<0.001) (online appendix eTable 3). MRI sequences employed also partly explained the heterogeneity in all studies, with a significantly higher pooled prevalence in studies using optimal sequences (<40 years p=0.027; ≥40 years p=0.002) (online appendix eTable 3). In studies with a mean age ≥40 years, a significantly higher prevalence was also observed in studies specifically excluding knees with radiographic OA (p<0.001) and in studies with a sample size ≥50 knees (p=0.029) (online appendix eTable 3).

Meta-analysis of the prevalence of BMLs. BML, bone marrow lesion.
Prevalence of osteophytes
Eighteen studies (3257 knees from 2499 participants) reported osteophyte prevalence with an overall pooled prevalence estimate of 25% (95% CI 14% to 38%; I2=98.2%). Studies with a mean age <40 years and ≥40 years had a pooled prevalence of 8% (0% to 25%) and 37% (22% to 53%), respectively, with significant evidence of between-study heterogeneity (I2=94.3% and 98.6%, respectively) (figure 5). The prevalence of osteophytes significantly increased with age (slope=10.2% increase per 10 years, 95% CI 1.7% to 18.7%, p=0.021) (online appendix eFigure 2) but not with a higher proportion of women (slope=−0.1% increase per 10% increase in proportion of women; 95% CI −4.8% to 6.5%, p=0.756). Although the relatively small number of studies precluded evaluation of some study level characteristics, in studies with a mean age ≥40 years prevalence of osteophytes was significantly higher in studies that specifically excluded knees with radiographic OA (p=0.046) (online appendix eTable 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis of the prevalence of osteophytes.
Compartment-specific outcomes
There were no significant differences between the prevalence of tibiofemoral and patellofemoral abnormalities (online appendix eTable 4). In studies with a mean age ≥40 years, medial meniscal tears (14% (95% CI 8% to 20%)) were significantly more common than lateral meniscal tears (5% (2% to 8%)) (p=0.009) (online appendix eTable 4).
Prevalence of secondary outcomes, sensitivity analysis and publication bias
The prevalence of secondary outcomes was generally assessed in fewer studies, with a large range of feature definitions (details in online appendix eTable 5). Prevalence of effusion/effusion-synovitis and subchondral cysts ranged from 0% to 92% (21 studies) and 0% to 24% (six studies), respectively. Prevalence of ligament tears was 0% for 16 of the 20 studies, with the remaining four studies reporting 1%–30% of mostly anterior cruciate or collateral ligament partial tears. Infrapatellar fat pad synovitis and oedema prevalence was 16%–80% (three studies) and 9%–75% (two studies), respectively. One study reported the prevalence of subchondral sclerosis/attrition, with a prevalence of 31%. Sensitivity analyses, excluding 21 studies of bilateral knees, resulted in almost identical prevalence of OA features as the full analyses (≤5% difference). Visual inspection of funnel plots stratified by age (<40 years and ≥40 years) revealed minimal asymmetry, with some evidence of small studies effect only for meniscal tears (Egger test <40 years of age p=0.027; ≥40 years of age p=0.037; online appendix efigure 4).
Discussion
This systematic review and meta-analysis of 63 studies involving 5397 knees demonstrated that OA features on MRI are common in asymptomatic uninjured knees and are generally associated with age. In young adults aged <40 years, the pooled prevalence of asymptomatic OA features ranged from 4% to 14%, with pooled prevalence estimates of 19%–43% in older adults. These findings assist both clinical providers and patients to interpret the importance of structural changes noted on MRI reports throughout the lifespan. Since more than one-third of the older population will exhibit these knee OA-related features, medical and/or surgical interventions targeting these imaging findings may not alleviate pain in patients with knee symptoms.
Clinical implications
Current management of OA-related features and atraumatic knee pain should centre on improving symptoms and functional limitations, and not be driven by imaging findings.79 80 The high rate of asymptomatic older adults (aged ≥40 years) with knee OA features on MRI helps to explain why interventions for these, such as arthroscopy, are no more efficacious in reducing symptoms than sham surgery.81 Imaging features also do not predict non-surgical treatment outcomes.79 The explosion of clinical MRI use and expenditure, by as much as 30% annually, over the past two decades1 2 has not resulted in improved treatment decisions or outcomes for people with knee pain in general practice settings.82 Alarmingly, in cases of back pain, undergoing early MRI has led to inferior outcomes.83 Future research should investigate whether explaining the normal rates of imaging features of OA to symptomatic patients presenting with imaging changes on MRI can improve outcomes and decrease the need for analgesic prescriptions, similar to that observed in the lumbar spine.84
The prevalence of MRI findings and older age
The prevalence of most knee OA-related features increased with older age, which partially explained the heterogeneity between studies. This increase of approximately 10%–15% per-decade for osteophytes and cartilage defects, and 3% per-decade for meniscal tears, suggests that these features reflect normal age-related changes. Indeed, meta-regression shows that approximately three-quarters of asymptomatic adults aged 70 years will have a cartilage lesion. A similarly high pooled prevalence of intra-articular abnormalities has also been observed in asymptomatic spines (disk/facet degeneration)85 and hips (cartilage/labral defects).86 Evidence purporting an increased risk of future radiographic OA in the presence of cartilage87 and meniscal pathology88 indicates that some of these asymptomatic OA features may not be entirely benign. As radiographic OA was already established in some knees in this review, it is possible that structural abnormalities observed were already part of the pathological OA process. However, higher rates of structural abnormalities were not evident in studies that potentially included knees with radiographic OA (ie, did not specifically exclude radiographic OA). Indeed, radiographic OA was also common in many asymptomatic knees and can also reflect normal ageing processes.89
BMLs and the association with physical activity
BMLs were the most common feature in younger adults and were not associated with age. Participation in weight-bearing sports contributed to the observed heterogeneity in BML prevalence in younger adults. The consequences of these BMLs in young athletes are not known. However, the transient nature of BMLs means that even after knee injury, when BMLs are common, most resolve without sequelae.90 While BMLs associated with established OA are an important source of knee pain, they display distinct biochemical properties from those associated with sports-related impact.91
The influence of MRI sequences acquired
The prevalence of OA features in the current review was influenced by the type of MRI sequences employed, reflecting variation in diagnostic accuracy with different MRI techniques.92 While MRI is the gold-standard imaging technique for diagnosing OA-related pathology,93 studies using non-optimal sequences to assess BMLs, such as gradient echo sequences, which are particularly prone to susceptibility artefacts,93 reported significantly lower rates. The pooled prevalence of meniscal tears in younger adults extends observations from a previous systematic review (without meta-analysis) describing the same prevalence (4%) of meniscal tears in asymptomatic, but not exclusively uninjured, athletes (mean age 20–47 years).94
Strengths and limitations
The studies included in this review used a large variety of outcome assessment tools to define MRI features. Although there were too many to assess their individual influence on prevalence rates, all methods to assess primary outcomes resulted in equivalent cut-off criteria. Thresholds to define presence of secondary outcomes were more variable and prevented meta-analysis. The detection bias associated with less experienced readers having more errors95 was reflected in risk of bias scores, with the addition of a specific item assessing reader experience. Risk of bias scores partly contributed to cartilage lesion prevalence between-study heterogeneity. In many studies, the asymptomatic uninjured controls were part of a comparator group for diseased cases; the general lack of publication bias (except for meniscal tears) confirms that prevalence rates reported were not a key determinant of publication.
Limitations of this review include the heterogeneity between studies that remained unexplained by the variables examined. Unexplained factors, such as the inherent subjective nature of grading MRIs, irrespective of experience, may contribute to OA feature prevalence. The influence of BMI was unable to be assessed as half of the studies did not report BMI. When whole knee data were not available, the highest prevalence from either compartment was analysed as the whole knee feature rate. While likely under-representing overall prevalence, this conservative approach ensured that a minimum rate was reported, as lesions in one compartment are known to increase the risk of lesions in the other compartment.96 Of the studies that reported compartment-specific abnormalities, prevalence of tibiofemoral and patellofemoral lesions were similar, while medial meniscal tears were significantly more common than lateral meniscal tears. Finally, the meta-regression analyses relied on aggregated published data, which may have underestimated the association of MRI features with older age and female sex.
Conclusion
In this systematic review, summary estimates of the prevalence of MRI features suggestive of OA among otherwise healthy asymptomatic uninjured knees ranged from 4% to 14% in young adults to 19% to 43% in older adults aged ≥40 years. These imaging findings must be interpreted in the context of clinical presentations and considered in clinical decision making.
What is already known on this subject?
Increasing availability of MRI has resulted in a rapid rise in its utilisation to help inform clinical management of patients with knee symptoms, yet the overall clinical benefit of the current use of knee MRI is uncertain.
Community-based studies have reported a high prevalence of knee osteoarthritis features detected by MRI, but these cohorts include people with knee pain and history of knee injury, a well-established risk factor for the accelerated development of knee osteoarthritis.
What are the new findings?
The prevalence of knee osteoarthritis features on MRI in otherwise healthy, asymptomatic, uninjured knees is high—up to 43% in adults aged ≥40 years.
Prevalence rates generally increase with age and are influenced by other factors such as physical activity levels and type of MRI sequences used.
References
Footnotes
Contributors AGC, BEØ and KMC: designed the study and planned the analyses. AGC and HFH: completed all searches and study selection (including inclusion and exclusion of abstracts). AGC and JJS: completed all data extraction. AGC and BEØ: completed all risk of bias assessment. AG: completed all critical appraisals of magnetic resonance imaging sequences. AGC: did the meta-analyses and meta-regressions, wrote the initial draft. All authors interpreted the data, critically revised the manuscript for important intellectual content and approved the final version of the manuscript.
Funding AGC was supported by postdoctoral funding from a European Union Seventh Framework Programme (FP7-PEOPLE-2013-ITN; 607510), and is a recipient of a National Health and Medical Research Council (NHMRC) of Australia Early Career Fellowship (Neil Hamilton Fairley Clinical Fellowship, APP1121173). HFH is supported by a NHMRC Project Grant (GNT1106852). JJS is supported by an Institutional DevelopmentAward (IDeA) from the National Institute of General Medical Sciences of theNational Institutes of Health (U54-GM104941). The funders had no role in any part of the study or in any decision about publication.
Disclaimer These sources had no involvement in study design, interpretation of data, writing of the manuscript or the decision to submit the manuscript for publication. All other authors declare no competing interests.
Competing interests AG is president of Boston Imaging Core Lab, LLC, and a consultant to Merck Serono, Genzyme, OrthoTrophix and TissueGene.
Provenance and peer review Not commissioned; externally peer reviewed.