Article Text

Abstract
Objective To analyse the relationship between the implementation of ‘the 11’ protocol during the regular season in a men’s amateur soccer team and the rate of hamstring and lateral ankle ligament (LAL) injuries, and to estimate the clinical benefit of the programme according to the type of injury and the position field.
Methods This cohort study was conducted in two different men’s amateur soccer teams. During two seasons, the exposed group (43 players) performed ‘the 11’ protocol twice a week, and the unexposed group (43 players) performed the regular training programme. All players trained three times per week for 1.5 hours per day. Data collection was performed for every 1000 hours of play.
Results 18 hamstring injuries (injury rate (IR) of 2.26 injuries/1000 training+competition hours) and 15 LAL injuries (IR of 1.88 injuries/1000) were registered in the exposed group. In the unexposed group, there were 25 LAL injuries (IR of 3.14 injuries/1000) and 35 hamstring injuries (IR of 4.39 injuries/1000). The number needed to treat to prevent one new case was 3.9 in LAL injuries, 3.31 in biceps femoris injuries and 10.7 in recurrent hamstring injuries.
Conclusions ‘The 11’ programme reduced the incidence of hamstring and LAL injuries in amateur players. According to the field position, the programme was effective for defenders and midfielders. In accordance with the type of injury, the exposed group had a lower risk of LAL, biceps femoris and hamstring injuries compared with those in the unexposed group.
- primary prevention
- athletic Injuries
- lower extremity
- sports medicine
- football
- soccer
Statistics from Altmetric.com
Introduction
Soccer (football) is one of the most popular sports worldwide and one of the most developed sports at both the professional and amateur levels.1 The most common medical procedure in sports focuses on recovery from injury to return to the preinjury level of athletic performance as soon as possible, but this process is costly.2–4 Soccer injury epidemiology provides worrying data. Andersen et al in 20031 also estimated an injury rate in soccer players ranging between 10 and 35 per 1000 game hours. In countries where soccer is practised consistently, in addition to the incidence of injury, the issue of public healthcare expenses must also be considered.5
According to Woods,6 hamstring injuries represent 12% of all soccer injuries and the 2006 study by Muller-Rath7 reported that the injuries in soccer players most commonly involved the lower extremities, with injuries to the ankle joint being the most prevalent. This same study concluded that professional medical treatment, with a focus on injury prevention, is justified in amateur or semiprofessional soccer. The hamstrings sustain a high incidence of injury in soccer and in all sports involving jumping and sprinting.8 This musculature, being biarticular, has an increased risk of injury due to its more explosive action, produced by the predominantly fast-twitch fibre component, and the high mechanical stress it experiences from the tension across two joints.9
The most common injury is to the ankle joint, mainly the external complex or lateral ankle ligament (LAL). Most ankle injuries are ligamentous and involve the lateral compartment. There is a very high incidence in soccer, especially involving the anterior talofibular ligament (ATFL), which has less load-bearing capacity when faced with forced inversion than the calcaneofibular ligament (CFL) and the posterior talofibular ligament.9
It is increasingly necessary to set protocols for action that ensure good medical attention at all levels to address the problems that soccer injuries arise, both during training and in competitions.10 Studies have been undertaken on the prevention of hamstring and LAL injuries in soccer, such as the 2003 trial by Askling et al 8 on the prevention of hamstring injuries conducted with elite Swedish soccer players, which achieved a 70% decrease in injuries. Other studies11–13 show that it is possible to reduce the incidence of injury, primarily joint and ligament damage, by performing preventive exercises based on proprioceptive training. Among current prevention strategies in amateur soccer, the protocol created by the Fédération Internationale de Football Association (FIFA) and its Medical Assessment and Research Centre (F-MARC) is applied in soccer as an injury prevention method. F-MARC developed ‘the 11’,14 a prevention programme for amateur players, the effectiveness of which has been widely demonstrated in a study carried out in Switzerland.15 ‘The 11’ is a simple, attractive, effective preventive programme that does not require any specific material, only a ball. The main objectives of this programme of 10 exercises are lumbopelvic or core stabilisation, plyometrics (jump training), agility and neuromuscular control.16 17
The Spanish soccer league comprises several interconnected leagues or divisions. The highest category is the first division, followed by the second division, second division B, third division and regional divisions. The latter are the amateur ranks and lowest tier of the Spanish league. They are organised by the regional federations that make up the Royal Spanish Football Federation. Everyone must be licensed and, based on the completed season results, the teams are promoted, relegated or remain unchanged.
Some studies18 report that soccer players in the top categories, who are better prepared, may have fewer injuries with respect to certain conditions and severity compared with amateur players who are not as well prepared. The objectives of this study were to analyse the relationship between the implementation of ‘the 11’ protocol during the regular season in a men’s amateur soccer team and the rate of hamstring and LAL injuries, and to estimate the clinical benefit of the programme according to the type of injury and the position field.
Materials and methods
An analytical observational retrospective cohort study was conducted in two different men’s amateur soccer teams in a soccer club of the Group VII of the first regional division of a Regional Football Federation in Spain.
This soccer club started to implement ‘the 11’ protocol twice a week in the presence of the team physiotherapist in 2010. Team players of 2008–2009 and 2009–2010 seasons were contacted by the team physiotherapist and were invited to be included in the unexposed group of the study. Team players of 2010–2011 and 2011–2012 seasons were also contacted by the team physiotherapist and were invited to be included in the exposed group of the study. Players who accepted met with the team physiotherapist to sign the informed consent and were enrolled consecutively.
Inclusion criteria were male amateur soccer players over 18 and under 40 years of age with a full medical record for the season studied, who at least attended 99% of training sessions and who gave signed informed consent. Exclusion criteria were: players who had previously participated in an injury prevention programme, who left the team before the end of the studied seasons or who suffered severe injury prior to the study. A player could not be included in both study groups. The institutional review board approved this study. Convenience sampling of players was performed to achieve an estimated sample size of 86 players, calculated for an injury prevalence in the unexposed group (UG) of 15% (data based on the observations of the team physiotherapist during the seasons prior to 2008). The magnitude of the RR to be detected was 3, assuming an alpha error of 5% (bilateral hypothesis) and a beta error of 10% (power: 1−beta: 90%). An ‘n’ of subjects in each group of 38 players (76 players) was estimated. Assuming a 10% loss gave us a total of 86 players: exposed group (EG): 43; UG: 43.
The EG performed ‘the 11’ protocol twice a week in the presence of the team physiotherapist during the 2010–2011 and 2011–2012 seasons, in accordance with the manual for implementing ‘the 11’ programme.14 17 19 The UG performed the regular training programme during the 2008–2009 and 2009–2010 seasons. All players trained three times per week for 1.5 hours per day with the same trainer.
Study outcomes under investigation were the following: (1) to determine the incidence of hamstring and LAL injuries and (2) to estimate the clinical benefit of the programme according to the type of injury and the position field.
To carry out this study, we reviewed the health database recording the health information of the participants during the course of the season, including data concerning the injuries experienced, both in competition and in training, and information relevant to the game and to ‘the 11’ programme. We collected data on sociodemographic variables (age, height and weight) and injury variables (LAL and hamstring injuries, position on the field, type of playing surface, time of injury, convalescence time, mechanism of injury and recurrence).
Definitions
Injury:8 Incident that occurs in a training session or game during the programme causing an absence at the next training session or game.
Recovery:14 When the player is able to play a game or fully comply with all instructions given by the coach (sprinting, turning, shooting, playing soccer).
Exposure: Time practising sports, both in training and competition, during which the player is susceptible to injury.
Recurrent injury or recurrence:14 An injury of the same type and in the same body part as the initial injury and that occurs up to 2 months after the player returns to participating in all activities after the initial injury.
Injury rate (IR) or incidence of injury: Injuries sustained during sporting activities, both in training and in competition, per 1000 hours of exposure.
Mechanism of injury: Incidental, sprint, collision, jumping, incorrect movement.
Injury time: When the injury occurred (practice: warm-up, training; or game: first half of game, second half of game).
Convalescence time: Number of days before normal resumption of training.
Type of playing surface: Natural or artificial grass, hard, wet when the injury occurs.
Field position: Playing position when the injury occurs (defender, forward, midfielder and goalkeeper).
Data collection was performed for every 1000 hours of play as this enabled us to compare our data with data from similar studies.19 20 To determine the number of training or competition injuries per 1000 hours, we calculated the IR. To obtain the IR per 1000 hours of exposure, we divided the number of injuries by the hours of exposure overall (7956 hours), in training (990 hours) and in competition (6966 hours) and multiplied by 1000.
The diagnosis and assessment of the injuries were performed by the team physiotherapist according to the F-MARC Football Medicine Manual.14 In the case of hamstring injury, during the examination the physiotherapist noted any tenderness of the injured area, pain on contraction and stretching, functional impairment or possible bruising. In LAL injuries, assessment was made of pain and swelling over the lateral malleolus and of all or part of the branches of the LAL, oedema, functional impairment, more intense pain with plantar flexion and inversion, and limited mobility. LAL stability was evaluated using two manoeuvres: the anterior drawer test to assess the integrity of the ATFL, and the inversion stress test to assess the ATFL and the CFL.
Statistical analysis
A descriptive and inferential statistical analysis was conducted to evaluate the clinical relevance. As a measure of association, the RR reduction (RRR) was examined and as measures of impact, the absolute risk reduction (ARR) and number needed to treat (NNT). Statistical significance or p value was estimated at p<0.05, and the 95% CI was also determined for all variables. In the multivariate analysis, the OR and its 95% CI were calculated. The SPSS statistical software (V.22.0) was used.
Results
The overall sample comprised 92 players, 6 of whom were excluded because they left the team before the end of the season. Thus, the final study involved 86 players, 43 in each cohort (figure 1). Seven of them were goalkeepers, 30 were defenders, 23 were midfielders and 26 were forwards. The sociodemographic variables are shown in table 1. Both groups were similar with respect to age, height and weight.
Sociodemographic variables analysis
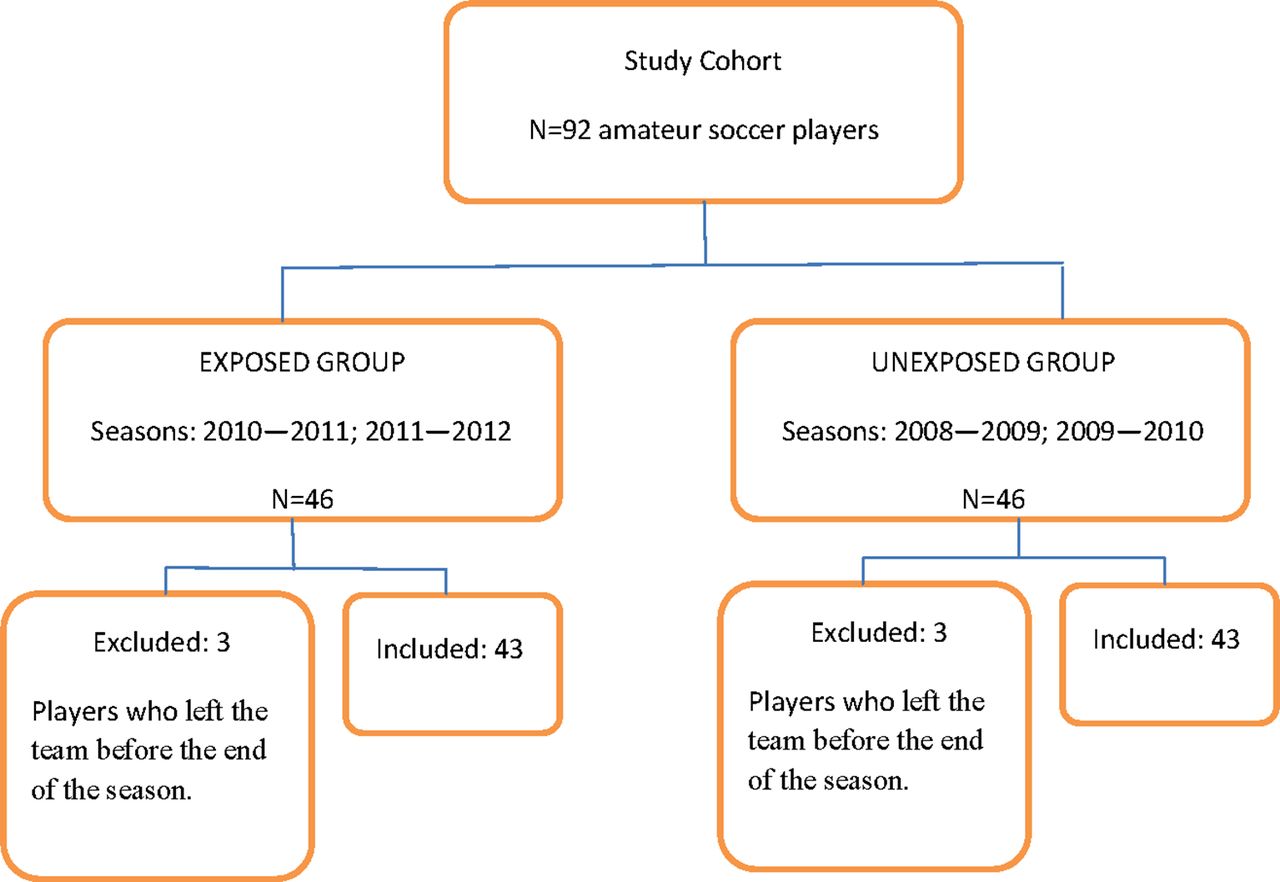
Flow diagram.
Descriptive analysis of LAL injury
During the 2010–2011 and 2011–2012 seasons, in the EG there were 15 LAL injuries (12 in training and 3 in competition), equivalent to an IR of 1.88 injuries/1000 training+ competition hours, 1.7 injuries/1000 training hours and 3.03 injuries/1000 competition hours. During the 2008–2009 and 2009–2010 seasons, in the UG there were 25 LAL injuries (18 in training and 7 in competition), equivalent to an IR of 3.14 injuries/1000 training+competition hours, 2.2 injuries/1000 training hours and 9.09 injuries/1000 competition hours (figure 2).
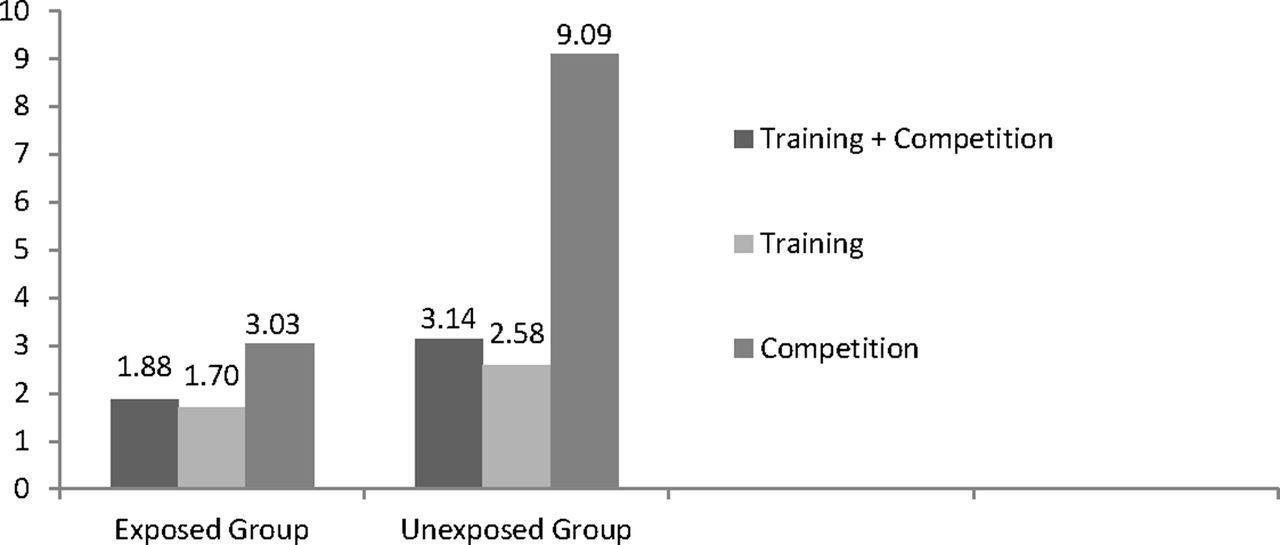
Incidence of lateral ankle ligament injuries for every 1000 hours of play.
Descriptive analysis of hamstring injury
During the 2010–2011 and 2011–2012 seasons, 18 hamstring injuries (9 injuries in training and 9 in competition) were registered in the EG, equivalent to an IR of 2.26 injuries/1000 hours, 1.29 injuries/1000 training hours and 9.09 injuries/1000 competition hours. During the 2008–2009 and 2009–2010 seasons, 35 hamstring injuries (16 in training and 19 in competition) were recorded in the UG, equivalent to an IR of 4.34 injuries/1000 hours, 2.2 in training and 19.9 in competition (figure 3).

{kind=link}
{kind=link}
{kind=link}
Incidence of hamstring injuries for every 1000 hours of play.
Regarding the total number of training or competition days missed due to the injuries studied, the EG missed a total of 568 days and the UG a total of 1143 days, representing a 50.4% increase. The average number of days missed was 13.2±19.2 days missed/player in the EG and 26.6±27.9 days missed/player in the UG.
Analysis of clinical relevance
Table 2 summarises the clinically relevant indicators of the effect of exposure to the exercise programme on the incidence of injury according to the player’s position. Regarding injury risk, a 49.67% decrease was seen in the defenders, a 39.2% reduction in the midfielders and no effect in the forwards.
Clinically relevant indicators of the effect of exposure to ‘the 11’ programme on the incidence of injury according to the player’s position and type of injury
Table 2 shows the programme’s effect on the type of injury. It was noted that the programme produced a 50% reduction in the risk of LAL injury and a 56.4% decrease in the risk of biceps femoris injury. When analysing recurrent injury, no effect was observed in LAL injury recurrence, though a 66.43% reduction in the risk of recurrence was seen in hamstring injury. The multivariate analysis was carried out by logistic regression analysis using the variables age, height, weight, field position and exposure (table 3).
Multivariate analysis
Discussion
The completion of ‘the 11’ protocol during the regular season of a men’s amateur soccer team significantly decreased the incidence of hamstring and LAL injuries. According to the field position, the programme was effective for defenders and midfielders with low NNT values. In accordance with the type of injury, the EG had a lower risk of LAL, biceps femoris and hamstring injuries compared with those in the UG.
Analysis of the results of the effect of exposure based on field position
Analysis of the clinical relevance indicators showed that the exposed defenders had about half the risk of injury as the unexposed defenders (see table 2). For every 100 exposed players, 38 injuries would be prevented and NNT indicated that we would prevent one injury for just three players exposed. The midfielders in the EG had a lower risk of injury than those in the UG. According to the NNT, treating three midfielders would prevent one injury. ‘The 11’ programme14 was not shown to be effective in preventing injury in forwards. This may be due to the characteristics of their game, as they spend much of the game in more static positions than their teammates, yet they are the most explosive in attack situations with the accompanying risk of hamstring injuries, as well as frequent contact situations with defenders on the opposing team. An interesting future study would be to analyse these players individually, together with their style of play, and adapt a special protocol for them because of their unique situation in the game.
Analysis of the results of the exposure on the type of injury
Analysis of the indicators of clinical relevance in LAL injuries showed that players in the EG had half the risk of LAL injury compared with those in the UG (see table 2). According to the NNT, one LAL injury would be prevented by treating. Regarding statistically significant variables, analysis of the biceps femoris injuries indicated that the players in the EG had a 56.5% lower injury risk than the players in the UG and NNT showed that treating four players would prevent one injury. Concerning clinically relevant indicators of hamstring injury recurrence, the EG players had a 66.43% lower risk of hamstring injury recurrence and 11 players would need to be treated to prevent one hamstring injury recurrence. Regarding LAL injury recurrence, we note that ‘the 11’ programme14 did not have a protective effect against recurrent LAL sprains. However, it was, though, very effective in decreasing the IR of primary LAL sprains. The possible reason might be the early return to the training. It is important to exercise caution with a player’s return to training following this type of injury, as many of the recurrences are likely related to returning to training or competition too soon rather than a lack of effectiveness of ‘the 11’ protocol.14
Regarding days lost, players exposed to ‘the 11’ programme14 had fewer days absent and suffered fewer injuries overall. The IR per 1000 hours of exposure (training and competition) showed a significant difference between the IR in training and competition, which demonstrates that competition is a factor that increases the IR, though this could also involve the presence of foul play that does not occur, at least not to the same extent, in training.
Multivariate analysis
The results (see table 3) indicated an absolute value of 3.10 (95% CI 8.33 to 1.15), signifying the risk of injury was three times lower for those players exposed to ‘the 11’ programme. The most statistically significant variable was ‘exposure’ to the ‘11’.
Comparison with other studies
Soligard et al 21 in 2008 conducted a randomised clinical trial in which the study population comprised young female amateur soccer players between the ages of 13 and 17. The intervention group performed the ‘11+’, and results showed a reduced risk of overuse injuries, severe injuries and overall injuries in the EG compared with the UG.
In 2010, Junge et al 15 conducted a cohort study to assess the implementation and the effects of a nationwide campaign to reduce the IR in amateur Swiss soccer players. The exposed teams carried out ‘the 11’ programme implemented by their coaches as a preventive measure against injuries and the unexposed teams performed the regular training. As a result, the exposed teams saw their incidence of injury reduced by 11.5% in games and by 23.5% in training compared with the unexposed teams. Unlike the study by Junge et al,15 in our study the programme was implemented by physiotherapists.
In 2015, Silvers Granelli et al 22 conducted a randomised controlled trial in which the study population comprised young male soccer players from the US National Collegiate Athletic Association Division I and Division II college soccer teams. The soccer players in the intervention group performed the ‘11+’ programme while those in the control group did not. There was an overall reduction of injuries in the intervention group by 46.1%, a decrease in time lost due to injury of 28.6% in the intervention group as compared with the control group and a NNT of 2.64. In our study, in addition to the NNT and the descriptive analysis, the risk of injury, distinguishing between training and competition per 1000 hours of exposure (rather than per 1000 players), was also analysed, enabling comparison with most similar studies.
The advantages of this study were the direct calculation of the incidence in the cohorts and that the recording and monitoring were conducted by a sports physiotherapist. In addition, our study calculated the clinical benefit of ‘the 11’ programme according to the position of the field and according to the type of injury, separately. However, this study has the inherent limitations of a retrospective study and other limitations, such as the selection bias that was controlled using inclusion–exclusion criteria, the random error that was controlled by calculating a 10% larger sample size for possible losses during follow-up and the information bias that was controlled by having the measurement of the variables performed in an appropriate manner and by a single investigator. To rule out fractures, scientific evidence has shown that x-rays are not always necessary. The Ottawa rules23 24 have proven to have adequate validity to rule out possible fractures. Regarding the selection of the prevention programme for this study, we think that ‘the 11’ programme covers the needs of this study. Although FIFA started the dissemination of ‘FIFA 11+’ in 2009,22 ‘the 11’ programme was used as a prevention programme in 2010 because it was better known.
‘The 11’ is a technique that is easy to implement in amateur soccer, is useful for the prevention of LAL and hamstring injuries, offers a good cost–benefit relationship and does not require special resources. This study, together with other similar studies and programs, demonstrates that injury prevention can and should be implemented in amateur or semiprofessional soccer to reduce the incidence of injury in both women and men.
What is already known on the subject
The injuries in soccer players most commonly involved the lower extremities.
To reduce the incidence of injury is possible by performing preventive exercises based on proprioceptive training.
The injury prevention method developed by FIFA and its Medical Assessment and Research Centre, ‘the 11’, reduces the incidence of injury.
What this study adds
The completion of ‘the 11’ protocol during the regular season of a men’s amateur soccer team significantly decreased the incidence of hamstring and lateral ankle ligament (LAL) injuries.
According to the field position, the programme was effective for defenders and midfielders with low number needed to treat values.
Those who perform ‘the 11’ protocol had a lower risk of LAL, biceps femoris and hamstring injuries compared with those who did not.
References
Footnotes
Contributors RN-G conceptualised and designed the study, coordinated and supervised data collection, drafted the initial manuscript and approved the final manuscript as submitted. CC-M conceptualised and designed the study, drafted the initial manuscript and approved the final manuscript as submitted. MRA-G coordinated and supervised data collection, critically reviewed the manuscript and approved the final manuscript as submitted. DO-B, VFG-G and AL-P carried out the initial analyses, reviewed and revised the manuscript and approved the final manuscript as submitted.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Miguel Hernandez University Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All availabe data from the study are reported in the submitted manuscript.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with ’BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.