Article Text

Abstract
Background Plantar fasciitis is a common cause of heel pain. The aim of this study was twofold: to compare steroid injection with placebo injection and to compare ultrasound guided with unguided steroid injection in the management of this condition.
Methods 65 patients with inferior heel pain were recruited between November 2008 and June 2011. Heel pain was measured using a visual analogue scale (VAS) at baseline and follow-up 6 and 12 weeks after injection.
Results 22 patients were randomised to ultrasound guided steroid injection, 21 patients to palpation guided steroid injection and 22 to ultrasound guided placebo injection. There was a significant difference in VAS scores between the groups at 6 and 12 weeks (p=0.018 and p=0.004, respectively). There was a 19.7 (95% CI 2.5 to 37.0) difference in mean VAS scores at 6 weeks between the ultrasound guided steroid group and the placebo group and a 24.0 (95% CI 6.6 to 41.3) difference between the unguided steroid group and the placebo group at 6 weeks. At 12 weeks, the mean difference was 25.1 (95% CI 6.5 to 43.6) and 28.4 (95% CI 11.1 to 45.7) respectively between both steroid injection groups and the placebo group. There was no difference in VAS scores following steroid injection between the ultrasound guided and the unguided groups at either time point. Plantar fascia thickness was significantly reduced after injection in both active treatment groups (p=0.00).
Conclusions In this study, steroid injection showed a clear benefit over placebo at 6 weeks and this difference was maintained at 12 weeks.
Trial Registration No ISRCTN79628180 (www.controlled-trials.com).
Statistics from Altmetric.com
Introduction
The plantar fascia is a thick, fibrous band of connective tissue deep in the skin on the sole of the foot. It is an important support for the longitudinal arch of the foot and acts as a shock absorber during walking and running.1
There is no widely accepted test for the diagnosis of plantar fasciitis.2 The presence of heel spurs on plain x-rays has been linked to heel pain but, in reality, this cannot confirm the diagnosis.3 MRI can visualise the plantar fascia but it is expensive and does not allow a dynamic assessment of the structures.4 Ultrasound is emerging as the preferred modality for imaging the plantar fascia and its insertion. It is non-invasive, radiation free, well tolerated and associated with a relatively low cost. Features on ultrasound which support the diagnosis include thickening of the plantar fascia and reduced echogenicity.5–,10 It is generally accepted that a plantar fascia thickness of >4–4.5 mm at its calcaneal insertion is diagnostic of fasciitis.3
Conservative treatment, with analgesics and rest, should be the first step in the management of plantar fasciitis. In those who fail to respond, steroid injection is often the next approach.1 ,11 ,12 Although steroid injection is practised widely, there are very few controlled trials of its efficacy in plantar fasciitis. One randomised controlled trial in 1956 found no statistical difference between injection of steroid and placebo in 22 patients.13 In another, more recent, trial of 106 patients, steroid injection was superior to placebo at 1 month but not at subsequent follow-up assessments.14 A recent BMJ Clinical Evidence report on various treatments for plantar fasciitis concluded that there was insufficient evidence to support the use of steroid injection and advised that they could be harmful in the medium to long term.15
Ultrasound guided injections have been recommended in patients who have failed to respond to unguided injections.16 There are few studies comparing ultrasound guided versus unguided steroid injections in plantar fasciitis and the outcomes have been inconclusive. Kane et al6 found no statistically significant difference in a group of 22 patients while Tsai et al17 reported that ultrasound guided injection prolonged the time to the recurrence of heel pain. Two other studies concluded that it was a safe and effective technique but used no control groups in support of this claim.18 ,19 Most of these studies involved small patient numbers.
The aims of this study were twofold: to compare steroid injection with placebo injection for the treatment of plantar fasciitis and to compare ultrasound guided with unguided steroid injection.
Methods
Recruitment
Ethical approval for the study was obtained from the Northern Ireland Research Ethics Committee (Ref: 08/NIR01/47). All participants gave their written informed consent prior to enrolment in the study. Patients were recruited between November 2008 and April 2011 from referrals to the Belfast Rheumatology Service. Follow-up continued until June 2011. Inclusion criteria were a history of heel pain combined with point tenderness over the medial tubercle of the calcaneus, and failure to respond to at least 8 weeks of conservative therapy. Exclusion criteria were a diagnosis of inflammatory arthritis, prior surgery or trauma to the heel, or a previous steroid injection into the heel pad.
Assessment
The baseline assessment included history taking, patient self-assessment of heel pain using a 100 visual analogue scale (VAS) and physician assessment of heel pain on palpation using a heel tenderness index where 0=no pain, 1=painful, 2=painful and winces, and 3=painful, winces and withdraws. These assessments were repeated at the follow-up visits, one at 6 weeks and the other at 12 weeks by a physician who was blinded to details of the patient's treatment group. An experienced podiatrist (HMcK) conducted a detailed biomechanical assessment of the foot using the foot posture index,20 which is a method of rating foot posture using set criteria and a simple scoring scale. A score is awarded for each of six parameters and the combined score gives a quantitative estimate of the overall foot posture. Positive scores of greater than +5 indicate a pronated foot posture while scores less than −5 indicate a supinated foot posture.
Ultrasonography
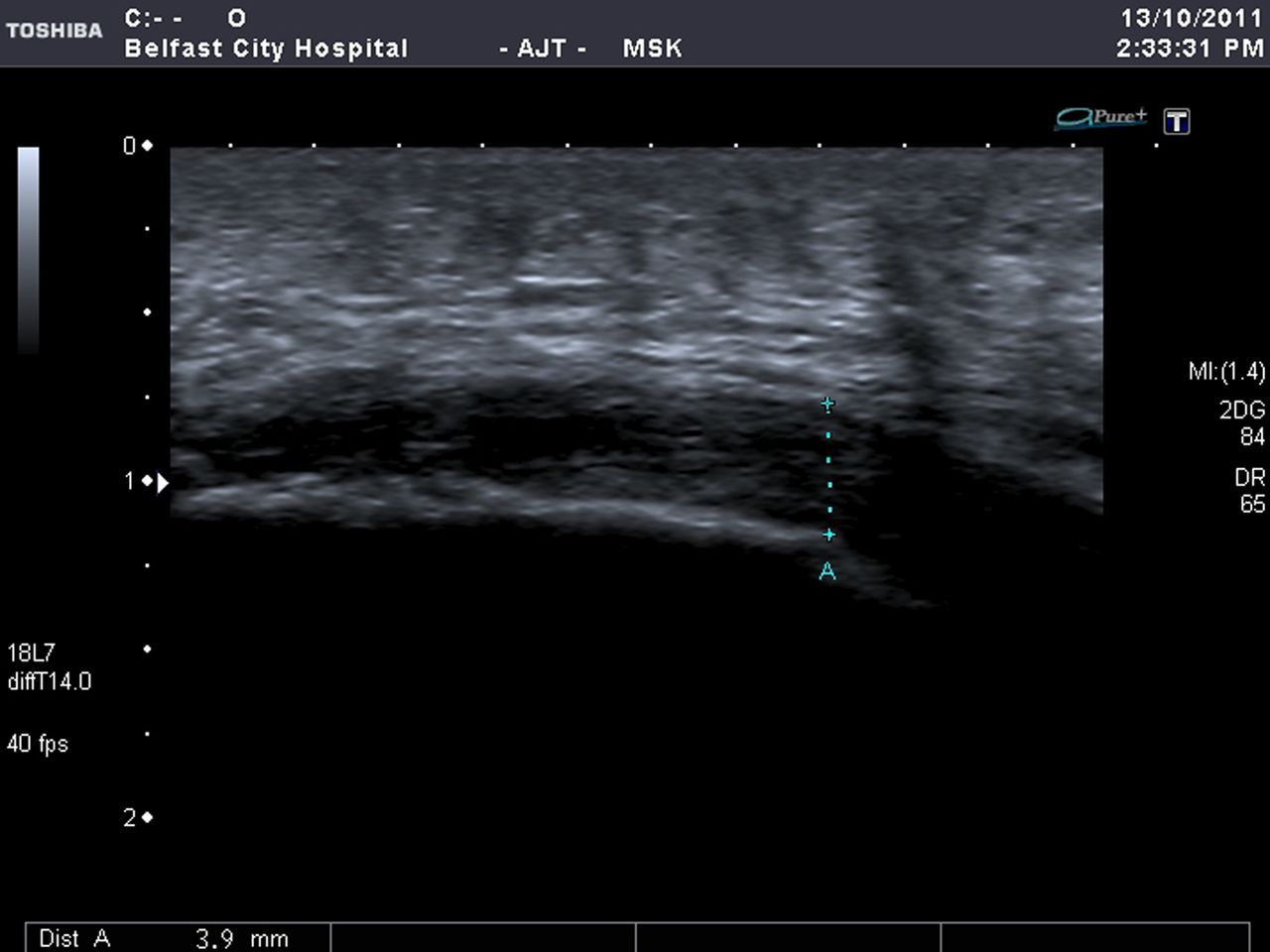
Musculoskeletal ultrasound was carried out by trained sonographers (WY, JB) who were blinded to the patient's medical history and podiatric assessment. Patients were examined lying in a prone position with their feet hanging over the edge of the couch. The plantar fascia was assessed using a 5–12 MHz linear probe positioned longitudinally over the medial tubercle of the calcaneus (Acuson Antares System, Siemens AG, Munich Germany) (see supplementary online image S1). The thickness of the fascia was measured with electronic callipers at a standard reference point: the proximal point of insertion of the fascia into the calcaneal tubercle18 ,21 (see figure 1 and supplementary online image S2). Plantar fascia thickness of >4.5 mm was considered abnormal.21–,23 The thickness of the heel pad was also measured at this reference point. Other sonographic observations included (a) the echoic character of the fascia, (b) the presence or absence of power Doppler signal at the enthesis (range 0–3)24 and (c) the presence of calcifications at the enthesis. Power Doppler settings were standardised with a pulse repetition frequency of 700 Hz and the lowest possible wall filter setting.

Ultrasound image showing the standard reference point for measurement of the plantar fascia thickness.
Intervention
Patients were randomised to one of three treatment groups in balanced blocks of six patients (http://www.randomization.com/) by an independent observer not involved in patient enrolment, who had sole access to the restricted randomisation generated. Ultrasound guided injections were carried out by a physician with extensive experience of the technique.
Blinding: Unguided injections were carried out under ‘sham’ ultrasound conditions to maintain patient blinding to the nature of the procedure; once the patient was comfortably lying in a prone position they could not visualise the ultrasound monitor or the injecting physician. The ultrasound probe was placed on their foot irrespective of which injection they were receiving. The physician performing these unguided injections was naive to the technique of ultrasound of the plantar fascia and had no prior experience of ultrasound guided injection. This was done in order to eliminate the potential bias from knowledge of ultrasound which can influence injection technique. The contents being injected were not identifiable to the injecting physician as an independent observer prepared the injections and covered the syringes with sterile masking tape in order to obscure the contents.
All injections were performed using the same approach via the posterior heel with the patient lying prone (see supplementary online image S3). Using an aseptic technique, the skin and subcutaneous tissues were anaesthetised with 2.5 ml of 2% lignocaine using a 25 mm 23 gauge needle.
Ultrasound guided injection
A 40 mm 21 gauge needle was inserted parallel to the heel pad in line with the long axis of the transducer (see figure 2). Either 0.5 ml (20 mg) of methylprednisolone acetate +0.5 ml of 0.9% saline (ultrasound guided steroid group) or 1 ml of 0.9% saline (placebo group) was injected along the superficial border of the plantar fascia enthesis under direct ultrasound guidance (see supplementary online video clip 1).

Ultrasound image showing the needle insertion in a longitudinal plane.
Unguided injection
Using an identical posterior approach, a 40 mm 21 gauge needle was inserted parallel to the heel pad in the direction of the medial tubercle of the calcaneus. An amount of 0.5 ml (20 mg) of methylprednisolone acetate and 0.5 ml of 0.9% saline was injected once the needle had been inserted to the hilt.
All patients were asked to avoid weight bearing on the heel pad for 48 h and were allowed to continue with their usual analgesia.
Outcome measures
The primary outcome measure was the patient's self-assessment of heel pad pain using the VAS pain score measured 12 weeks after the injection. Secondary outcome measures included the VAS pain score at 6 weeks, changes in the plantar fascia thickness measured by ultrasound and heel pad tenderness measured by the physician-assessed heel tenderness index, both at 6 weeks and 12 weeks.
Repeat injection
Any patient who failed to respond clinically to injection at 12 weeks was then offered an ultrasound guided steroid injection outside the trial.
Statistical methods
Baseline summary statistics were described as mean (SD) or median (IQR) if data were heavily skewed. Sample size of 22 patients per group was calculated to permit the detection of differences of 20 mm in the mean post-treatment VAS scores between the groups (90% power, p<0.05, two-tailed) assuming an SD of 22 mm and a patient dropout rate of 10%.
The main outcome variables were assessed at 6 weeks and 12 weeks using analysis of covariance with the baseline values as a covariate. Sensitivity analysis was conducted using imputation to calculate the impact of missing values but this led to no changes in the conclusions.
Multiple regression analysis was used to evaluate potential associations between the baseline clinical characteristics or sonographic features and the VAS pain responses. No significant associations were found. Statistical analysis was performed using IBM SPSS Statistics (V.19).
Results
Figure 3 provides a summary of recruitment. In all, 86 referrals were screened of which 73 fulfilled the inclusion criteria and were invited to participate. Overall, 65 patients were enrolled into the study (29 male and 36 female). Of these, 22 patients received an ultrasound guided steroid injection, 21 an ultrasound guided saline (placebo) injection and 22 an unguided steroid injection.

Flow diagram showing patient recruitment.
Study withdrawals
Two patients in the ultrasound guided steroid injection group dropped out after assessment at 6 weeks because of persistent heel pain. One had a baseline plantar fascia thickness of 9 mm and their pain settled after a repeat steroid injection at 12 weeks. The other patient had severe heel pain at 6 weeks and was fitted with an air-cast boot to prevent direct weight bearing on the heel. This patient also had a repeat steroid injection at 12 weeks after which the pain subsided. A third patient who withdrew from the study was in the unguided steroid group. She dropped out at 10 weeks due to problems with transport but completed a VAS score by telephone.
Four patients in the ultrasound guided steroid group were lost to follow-up at 12 weeks. Two patients in the placebo group were lost to follow-up at 6 weeks and one at 12 weeks.
Baseline characteristics
The mean (SD) age of the participants was 49 (11.3) years with a median (range) duration of symptoms of 6 (2.5–60) months. The mean (SD) body mass index (BMI) was 31.6 (5.2) and 59/65 patients had a BMI>25. The characteristics of the groups are summarised in table 1.
Baseline clinical, sonographic and biomechanical features
Sonographic features
The mean (SD) baseline thickness of the plantar fascia was 6.1 (1.5) mm. and in 27 patients (42%) the fascia was hypoechoic. A total of 16 patients (25%) had a positive power Doppler signal at the plantar fascia enthesis and in 13 patients (20%) there were microcalcifications within the fascia.
Podiatric assessment
There were no significant differences in the biomechanical foot posture index scores between the three groups. In all, 44 patients (68%) had a pronated foot and three (5%) had a supinated foot.
Overall, 53/65 patients had a lateral x-ray of their affected foot and 50% of these showed the presence of a small calcaneal spur.
There was no significant difference in any baseline characteristic between the three groups.
VAS scores
The mean (SD) post-treatment VAS scores at 6 weeks were 33.1 (28.4) in the ultrasound guided steroid injection group, 30.3 (27.3) in the unguided steroid injection group and 50.9 (31.4) in the placebo injection group. The VAS scores at 12 weeks were 28.4 (24.9), 28.2 (24.8) and 53.8 (33.8), respectively.
Analysis of covariance revealed significant differences in mean VAS scores between the three groups at 6 weeks (p=0.018) and at 12 weeks (p=0.004). There were no significant differences (p=0.58) between the steroid treatment groups at either time point but individual comparison of each of these active treatment groups with placebo showed significant differences at both 6 weeks and 12 weeks (see table 2).
Outcome measures
Heel tenderness index scores
The physician-assessed heel tenderness index scores showed no statistical difference between the active treatment groups at either 6 or 12 weeks. The difference between the ultrasound guided steroid injection group and the placebo group was insignificant (p=0.08) at 6 weeks but significant at 12 weeks (p=0.002). The difference between the unguided steroid group and the placebo group was statistically significant at both time points (p=0.0062 and 0.001).
Plantar fascia thickness
Plantar fascia thickness was significantly reduced after injection in both active treatment groups (p=0.00, one-way analysis of covariance). The mean (SD) reduction at 6 weeks was 1.4 (1.1) (95% CI 0.9 to 1.90) mm in the ultrasound guided steroid group and 1.4 (1.1) (95% CI 0.95 to 1.92) mm in the unguided steroid group. In the placebo group, the reduction in thickness was 0.25 (0.6) (95% CI 0.01 to 0.52) mm (see figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reduction in plantar fascia thickness at 6 weeks. US, ultrasound.
One patient (5%) in the ultrasound guided group and six (27%) in the unguided group required a repeat steroid injection at 12 weeks compared with 11 (52%) patients in the placebo group (p=0.002).
There were no adverse events as a result of any of the interventions.
Discussion
This is the first placebo controlled study to show a sustained benefit from steroid injection of the heel pad over a 12-week period in the treatment of inferior heel pain. Patients in both the ultrasound guided and unguided injection groups showed a statistically significant reduction in VAS pain scores when compared with the placebo group. There were also significant reductions in the physician-assessed heel tenderness index and the plantar fascia thickness in both active treatment groups.
The study was conducted on patients with simple mechanical heel pain. We deliberately excluded patients with a prior history of inflammatory arthritis or enthesitis and those who had had a previous heel injection. This study design allowed us to draw conclusions on the benefits of treatment in a subgroup that represents the commonest pattern of heel pain but it would be unwise to apply these findings to other groups. One of the advantages of musculoskeletal ultrasound is its ability to detect subtle signs of inflammatory enthesopathy in patients who present with heel pain.
There were no significant differences in the baseline clinical characteristics of the three treatment groups. The preponderance of females is in keeping with previous reports25 ,26 as is the elevated mean BMI of the group.27
All of our patients underwent detailed assessment by an experienced podiatrist (HMcK). Biomechanical abnormalities are known to be important risk factors in many patients with heel pain but we were unable to demonstrate a significant association between the foot posture index and the response to injection. In this study, 47 out of 65 patients (72%) had biomechanical foot abnormalities with overpronation being the most common problem (44 patients/68%). These results are not surprising and support the findings from previous studies.3 ,28 ,29
The significance of calcaneal spurs in patients with plantar fasciitis has been questioned for some time.3 ,30 ,31 The high prevalence of calcaneal spurs in asymptomatic patients raises questions about the importance of this finding.32 While there is no doubt that small subcalcaneal heel spurs are commoner in patients with inferior heel pain,3 their presence in an individual patient is of little diagnostic value and changes in the plantar fascia thickness are of much more importance.33
In recent years, musculoskeletal ultrasound has become part of the routine clinical practice of many rheumatologists.34 It is a powerful tool for evaluating joint and soft tissue pathology and for facilitating interventions such as joint aspiration and steroid injection. The use of ultrasound to localise joint and soft tissue fluid collections significantly improves the rate of diagnostic aspiration, particularly in small and medium-sized joints.35 ,36 There is conflicting evidence regarding the benefits of ultrasound guided joint injections and relatively few studies, to date, have looked at patient reported outcome measures.37 A recent study showed that ultrasound guidance significantly improved pain scores and overall response in a variety of joint injections38 and a positive response to ultrasound guided shoulder injection has also been reported.39 In contrast, another study demonstrated a significant improvement in the accuracy of injection with ultrasound guidance but without an improvement in clinical outcome.40
Despite demonstrating the clear superiority of steroid over placebo injection, we failed to show a difference in clinical outcome between ultrasound guided and unguided steroid injection. This could have been due to a number of factors but, most likely, the diffusion of corticosteroid in the vicinity of the injection site meant that it was not essential to place the needle in a precise spot in order to achieve the desired clinical benefit. A systemic effect of the corticosteroid is another way in which both active injections could have produced their benefits. This was the conclusion of a study by Ekeberg et al who looked at subacromial ultrasound guided steroid injection versus an intramuscular steroid injection and found that they were equally effective.41
While ultrasound guidance may not be essential to success in heel pad injection, it provides a lot of useful information during the clinical consultation that influences decisions about patient management.42 We chose to inject the steroid through the back of the heel along the superficial border of the plantar fascia enthesis because this is less traumatic than injecting directly into the fascia itself but there is no general consensus as to the correct way of performing the procedure.
Plantar fasciitis has been described as a self-limiting condition which will eventually resolve regardless of treatment.25 ,26 Nevertheless, the condition can cause significant pain and disability for weeks and months and so when conservative measures fail to resolve the problem, it is important to know that steroid injection (whether guided or unguided) can have significant benefits in the short and medium term.
In conclusion, we believe that the results of this study provide the first robust evidence supporting the use of a single steroid injection of the plantar fascia for the treatment of inferior heel pain that has failed to respond to conservative treatment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online legends
- Data supplement 2 - Online figures
- Data supplement 3 - Online video
{kind=link}
{kind=link}
{kind=link}
Footnotes
-
Contributors All authors contributed significantly to the study and had full access to the dataset and statistical reports. EB: study coordinator, protocol design and guided injections; HMcK: podiatric assessments; JB: patient recruitment and ultrasound; WY: ultrasound assessments; OM: patient recruitment and guided injections; CB and JF: unguided injections; CP: statistical advice; GW: study design; and AT: study design and guarantor.
-
Funding No external funding was received.
-
Competing interests None.
-
Patient consent All patients provided written informed consent.
-
Ethics approval Ethics approval was provided by the Northern Ireland Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.