Article Text

Abstract
Background Concussion is one of the most commonly occurring injuries in sport today. The Sport Concussion Assessment Tool (SCAT) is a commonly used paper neurocognitive tool. To date, little is known about SCAT baseline normative values in youth athletes.
Objective The purpose of this study was to determine normative values on the SCAT for male and female youth hockey players.
Methods This is a secondary data analysis of pooled data from three prospective cohort studies examining the risk of injury in paediatric ice hockey players aged 9–17 years. A preseason baseline demographic and injury history questionnaire was completed by each player.
Results A total of 4193 players completed SCATs at baseline and were included in the analysis. 781 players (18.6%) reported a previous history of concussion. Fatigue and low energy followed by headache were the most commonly reported symptoms in all players. The majority of youth players could recite all five words immediately but only three words when delayed. A smaller proportion of the males were able to report the months of the year in reverse order compared with females of a similar age. The median number of digits recited in reverse order was 4.
Conclusions Youth ratings varied between age groups, gender and from previously reported ratings of varsity athletes, possibly reflecting developmental and gender differences. An understanding of these differences in youth athletes is important to ensure appropriate performance expectations on the SCAT and when making clinical decisions following a concussion.
Statistics from Altmetric.com
Concussion is a commonly occurring injury in sport today and has been reported to account for the greatest proportion of all injury types in youth ice hockey.1,–,3 Concussion is defined as ‘A complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces.’4 A wide array of symptoms and signs can occur following a concussion, including clinical symptoms, physical signs, behavioural alterations, balance disturbance, altered sleep and altered cognition.4 The majority of individuals recover within 7–10 days, but some individuals are left with prolonged symptoms.4
The Sport Concussion Assessment Tool (SCAT) is a paper neurocognitive tool that was initially developed at the Second International Conference on Concussion in Sport in Prague in 2005 by combining existing tools.5 It has established face validity, but reliability and change scores have not been reported to date.6 It was developed for patient education in addition to physician assessment in individuals who have sustained a sport-related concussion. The SCAT has been reported to be suitable for use in athletes down to the age of 10 years.4
The SCAT consists of both a subjective and evaluative portion. The subjective portion consists of 25 symptoms that the athlete rates based on how they feel at the time of administration on a seven-point Likert Scale of 0–6, with 0 representing no symptoms and 6 representing severe symptoms.5 The evaluative portion of the SCAT includes signs, modified Maddocks questions, symptom score, a cognitive assessment and neurological screening.5 The cognitive assessment includes recall of five unrelated words immediately upon hearing them (immediate word recall) and again following concentration tasks (delayed word recall), stating the months of the year in reverse order and repeating single digits in reverse order (starting with three to a maximum of six digits).5
Knowledge of an individual's score on a measure when they are not injured will give a baseline normative value for that specific individual for comparison at the time of injury. Similarly, normative information from a target population is of value when determining if an individual varies from the population score and provides context for the test to be interpreted. Shehata et al7 reported normative values on the SCAT for varsity athletes. The SCAT2 is a newly developed tool that expands on the objective elements in the SCAT.4 Although the SCAT is a widely used tool, normative values for children and adolescents are not currently known.
The purpose of this study was to determine the normative values on the SCAT for 11–14-year-old male hockey players and 9–17-year-old female hockey players.
Methods
This study is a secondary data analysis of pooled data from three prospective cohort studies examining the risk of injury in paediatric ice hockey players (male Pee Wee (11–12-year-olds), male Bantam (13–14-year-olds), female Atom (9–10-year-olds), female Pee Wee (11–12-year-olds), female Bantam (13–14-year-olds) and female Midget (15–17-year-olds)).2 8 9 The studies took place in community ice hockey arenas in Calgary, Edmonton, Quebec City and Montreal. All studies used the same prospective injury surveillance system, previously validated in youth ice hockey.10 In the initial prospective cohort studies, subjects were randomly selected to participate by team for the male studies, and an inclusive sample was used for the female portion of the study. Parental and player written consent was required prior to participation. Individuals who consented to participate in the above studies and completed a baseline SCAT were included in the secondary data analysis. Females playing in the mixed league were included in the female analysis. Individuals were excluded if previous concussion status was unknown. On the mixed teams, subjects were excluded if gender was unknown. Individuals were excluded if they were concussed at the time of SCAT completion. As only active players were included, no one was excluded based on this criterion.
Participants
Male participants
Pee Wee
One hundred and fifty-two teams were randomly selected, and a total of 2154 individuals aged 11–12 years consented to participate in the study during the 2007–2008 hockey season. These teams represented the top 60% of players by level. There were 33 females in this data set, and they were moved to the female analysis. Eleven individuals were excluded based on unknown gender, and no subjects were excluded based on an unknown previous history of concussion (PC). A total of 2049/2121 (96% of the total sample) completed a SCAT at baseline and were included in this portion of the study.
Bantam
One hundred and thirty teams were randomly selected, and a total of 1971 individuals aged 13–14 years consented to participate in the study during the 2008–2009 hockey season. These teams represented the top 30% of players by level. Fourteen females were moved to the female analysis. Five individuals were excluded based on unknown gender, and 32 were excluded due to an unknown previous concussion history. A total of 1831/1971 (92.9% of the total sample) completed a SCAT at baseline and were included in this portion of the study.
Female participants
Twenty-eight female youth hockey teams were included in this sample, and a total of 324 females ranging in age from 9 to 17 years consented to participate in the study. Four Atom teams (9–10 years), six Pee Wee teams (11–12 years), nine Bantam teams (13–14 years) and nine Midget teams (15–17 years) participated in the study. Forty-seven females playing on mixed teams were included in this analysis for a total of 371 girls. Twenty-five individuals had an incomplete past concussion history and were excluded. Thirty-three of the remaining participants did not have a complete SCAT at baseline. A total of 313/371 subjects (84.4% of the total sample) completed a SCAT at baseline and were included in this portion of the study.
Procedures
Each player completed a baseline preseason questionnaire that included questions about demographics, past concussions, previous injury and sport participation history. It is often recommended that parents and/or teacher input also be sought to gather all relevant information.11 To ensure that all relevant information was collected, the SCAT was taken home for the subjective portion to be completed with parental assistance in the female Atom group. For all other groups, the SCAT was administered during a practice or prior to a game. If the player requested parental input, this was included in the SCAT. Each team was assigned a team therapist (either a physiotherapist or athletic therapist) who was trained to administer the SCAT and followed the team over one season of play. At the beginning of the season, the team therapist completed the evaluative portion of the SCAT with each player.
Analysis
A descriptive analysis of both the subjective and evaluative portions of the SCAT was performed. For each group of athletes, values were stratified based on PC to determine if baseline values differed. For ease of comparison, descriptive statistics similar to those reported by Shehata et al7 were used. Median and mode total symptom scores were calculated, and the percentage of athletes reporting no symptoms was calculated for each group. The proportion of players reporting each symptom for each age group and gender based on past concussion history was determined. The proportional distribution of the sample for each value of immediate and delayed recall (0–5), digits in reverse order (0–6) and number of months of the year recited in reverse order (0–12) was also calculated.
All subjects and their parents provided written consent to participate in the study. This study is a secondary data analysis of studies that have previously obtained ethics approval from the Office of Medical Bioethics at the University of Calgary.
Results
A total of 4193 subjects met the inclusion criteria for participation in the study. Baseline SCAT results were stratified based on PC, age group and gender. The female groups were initially analysed as a group, but once stratified by age group, differences were noted among groups, so the stratum specific age values rather than the crude estimates are presented.
A summary of the total symptom score of the SCAT for each group is presented in table 1. Only the Midget females with a PC had a mode total symptom score greater than zero.
Total symptom score by age group and previous concussion history
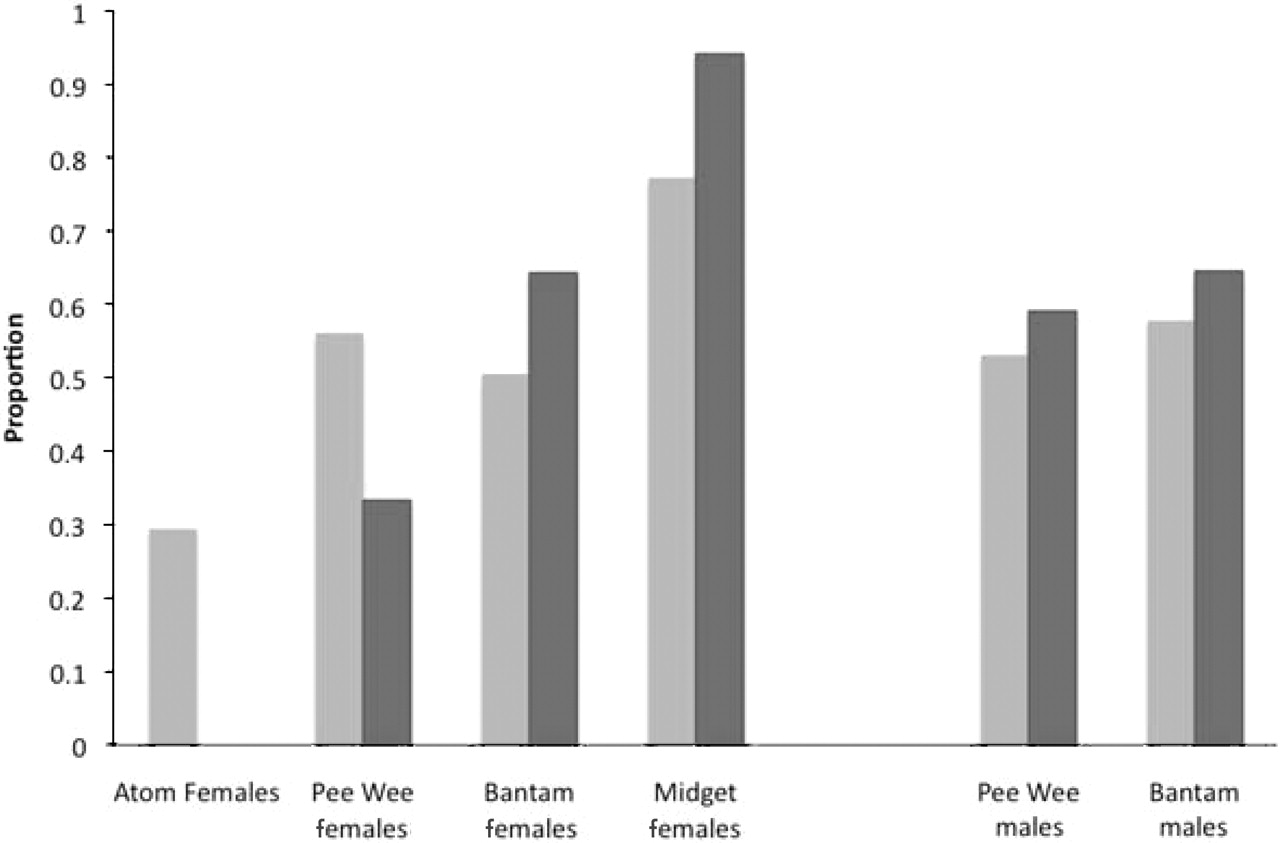
The proportion of players reporting at least one symptom is presented in figure 1. In all groups except for the Atom and Pee Wee females, a higher proportion of PC athletes reported symptoms than those who had not previously been concussed (NC). The PC and NC Midget females had the highest proportion of the sample reporting symptoms (94.1% and 77.3% respectively). The Atom females (PC and NC) had the lowest proportion of the sample reporting symptoms (0% and 29.4%).

{kind=link}
Proportion of subjects with symptoms. Light grey, no previous history of concussion; dark grey, previous history of concussion.
The percentage of individuals reporting each of the five most common symptoms for each stratum specific group is presented in table 2. In some groups, there were ties for the fifth most common symptom, so more than five may be presented. Only one subject in the Atom females reported a PC, and she did not report any symptoms, so this group is excluded from the table. For all groups, fatigue or low energy was among the top five symptoms reported. All groups except PC Pee Wee females had trouble falling asleep as one of the top five most commonly reported symptoms.
Percentage of sample reporting the most common symptoms
The objective results of the SCAT are in table 3. All groups had a median of five words recalled immediately. The majority of groups had a median of three delayed words recalled. There was a range of responses from 0 to 5 words in nearly all groups. The Atom females were not asked to recite the months of the year in reverse order due to age. For the NC Pee Wee females, only a small proportion of the sample was able to complete this task (40.5%). However, in PC Pee Wee females, all players were able to complete this task (n=3). The majority of the older females (Bantam and Midget) were able to recite all of the words in reverse order (>70%), but only half (46.6–53%) of the males could complete this task. The median number of digits recalled in reverse order was 4 in all cases except for the NC Midget females who could recall a median of 5 words.
Evaluative portion of Sport Concussion Assessment Tool: by age group and concussion history
Discussion
Little is known about the normative baseline SCAT scores in youth ice hockey players, despite concussion being a commonly occurring injury in youth ice hockey and the SCAT a commonly used tool. In our study, SCAT symptoms and scores varied by age and gender, and differed from those previously reported in varsity athletes.7 Children and adolescents are different from adults cognitively, behaviourally and structurally.12 They are growing and developing, facing different challenges than adults, and normative values on outcome measures may also be different, as was demonstrated in this study.13 14 Baseline normative values on the SCAT are important in order to understand symptomatic and cognitive changes that may occur following a concussion.12
Subjective SCAT
To date, only one study has examined the baseline normative values on the SCAT.7 Shehata et al7 reviewed the baseline SCAT scores of 260 varsity collision sport athletes with a mean age of 20.5 years. In their sample, a greater number of females reported symptoms than males (75.7% and 52.6% respectively). These values varied in our study. Of note, the proportion of Pee Wee females with a PC reporting symptoms (33.3%) was lower than Pee Wee males (59.1%). However, PC Bantam females and males had nearly equal proportions reporting symptoms (64.3% and 64.5% respectively). The proportion of Pee Wee males reporting symptoms is similar to that reported in varsity athletes, but the proportion of Bantam males reporting symptoms at baseline is slightly higher. The Atom females had the smallest proportion, with symptoms and the Midget females the greatest proportion, illustrating a trend toward increased prevalence of symptoms with increased age in the females. Nearly all of the PC Midget females reported symptoms (94.1%). NC Midget females without a PC had a similar proportion of symptoms to varsity females (77.3%).
The findings on the subjective portion of the SCAT were right-skewed, with many individuals scoring zero. Individuals with a PC had a tendency toward higher total symptom scores. For the Midget females, this appears to be an age where symptoms are felt at times when the players are not concussed, and an elevated baseline symptom score is common. Only a very small proportion in this group with a PC (5.9%) did not report symptoms.
Many symptoms listed on the SCAT are not specific to concussion and may also be present in an uninjured population.15 16 An understanding of the normally occurring prevalence of these symptoms is important when looking at a difference incurred by a concussion.12 Shehata et al7 found that fatigue or low energy was the most commonly reported symptom for males and females irrespective of concussion history.7 For all groups reporting symptoms, fatigue or low energy was among the top five reported symptoms in the current study, and was the number one symptom reported by all groups except the PC Bantam females, PC Midget females and PC Pee Wee males where headache was the most commonly reported symptom. Headache is among the most commonly reported symptoms following a sport-related concussion.17 18 Differing reports of awareness of return to play guidelines have been reported,17 19 and it is possible that athletes had returned to play with a postconcussive headache or other symptoms. Very few individuals checked ‘other’ on the symptom checklist. Thus, it appears that the symptom checklist encompasses the majority of symptoms.
Objective SCAT
The majority of subjects were able to recall five words immediately. This is similar to findings by Shehata et al.7 The median delayed word recall in the present study was 3 for most groups, which differs from the median seen in varsity athletes of 4.7 The vast majority of varsity athletes were able to correctly complete the months of the year in reverse order (89.9–96.7%),7 whereas in our study only the two oldest female groups could complete this with relatively high success (70.0–82.4%). The PC Pee Wee females were all able to complete this task successfully. All male groups could complete this task approximately half of the time, possibly representing a gender difference. The median number of digits recited in reverse order was 4 for all groups except the NC Midget females, who had a median of 5 digits. This is less than the median of 6 for females and 5 for males, observed in varsity athletes.7 The differences seen in this study compared with the varsity study may reflect a developmental difference.
Limitations
This study has some limitations. It was assumed that no players had sustained an unreported concussion. A differential misclassification bias may have occurred, resulting in an underestimation in differences between groups if undiagnosed concussions occurred. Players who had previously sustained a concussion may be more aware of their symptoms and have a self-reporting differential measurement bias toward increased symptoms, since they had previously experienced symptoms and were able to recognise them (eg, many youth may not be able to recognise ‘dizziness’). All therapists attended a training session to facilitate consistent administration of the SCAT. An environment free of distractions and maximal effort was assumed during administration of the SCAT but may not have always been possible. The male participants in the study were independently recruited in consecutive years. Some of the players from the Bantam cohort may have also participated in the Pee Wee cohort. We were unable to determine if any players participated in both years of the study due to identity concealment. Due to the year between SCAT completions, a decay in learning effect is expected to have occurred, decreasing the likelihood of any learning effect on the SCAT scores. As this study only included ice hockey players aged 9–17 years, the generalisability to other sports and ages is limited. Previous concussion history was coded as yes or no, so the number of past concussions was not known.18
The SCAT has recently been revised and expanded in the SCAT2.4 There are many consistencies between the SCAT and SCAT2. Symptoms not included on the SCAT2 include hearing problems, feeling dinged or dazed, sleeping more than usual and other. Dizziness and balance problems are individually reported, rather than jointly. A modified Balance Error Scoring System, three trials of the immediate word recall and a rating for each element, up to a total score of 100, are all additions to the SCAT2.4 Thus, many of the findings from the current study also apply to the SCAT2.
Conclusions
This study is the first to report baseline SCAT values in a paediatric population. A greater number of baseline symptoms were reported by Bantam and Midget females. There was a tendency toward higher total symptoms reported in individuals with a PC. Overall fatigue and low energy followed by headache were the most commonly reported symptoms in all players. Headache was the symptom most commonly reported in groups with a PC. Youth scores on the evaluative portion of the SCAT have not been previously reported and are summarised here.
Reported baseline values on the SCAT differed from that previously reported in varsity athletes. This has an impact on clinical practice, as one must be aware of baseline differences in youth athletes to ensure appropriate performance expectations on the SCAT and when making clinical decisions following a concussion. Baseline testing in youth athletes will allow comparison with an individual's baseline score following a concussion. The SCAT may need to be repeated regularly due to altered stages of development which may affect performance. However, the possibility of a learning effect must also be considered. The ability of a youth athlete to complete the objective portion of the SCAT may differ from an adult. Initial symptoms reported may be due to developmental differences, not injury. Future research should examine the consistency of these findings across other ages and sporting groups.
What is already known on this topic
Baseline normative values on the Sport Concussion Assessment Tool (SCAT) are available for varsity athletes but not youth athletes. The SCAT is a widely used tool for assessment following a concussion and in the clinical decision-making process for return to play.
What this study adds
Baseline normative values on the SCAT have not previously been available for youth athletes. Norms for this population will provide a platform for comparison during times of injury and provide context for baseline testing in youth athletes. Variation was observed across genders and age groups.
Acknowledgments
The authors acknowledge the support of research coordinators and research assistants J McAllister, G Hamilton and M Decloe. Thank you to all the players, parents and coaches who participated in these studies and share a similar vision in preventing injuries in youth ice hockey. Without the collaborative efforts of Hockey Canada, Hockey Calgary, Hockey Edmonton and Hockey Quebec, this work would not have been possible.
References
Footnotes
-
Funding These studies were funded by the Canadian Institutes of Health Research, Max Bell Foundation and Alberta Centre for Child, Family and Community Research. KJS is funded by an Alberta Heritage Foundation for Medical Research Doctoral Award. CAE is funded by a Canadian Institutes of Health Research New Investigator Award, Alberta Heritage Foundation for Medical Research Population Health Investigator Award and a Professorship in Pediatric Rehabilitation funded by the Children's Hospital Foundation through the Alberta Children's Hospital Research Institute for Child and Maternal Health.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was provided by the Office of Medical Bioethics, University of Calgary.
-
Provenance and peer review Not commissioned; externally peer reviewed.