Article Text

Abstract
Introduction Tendinopathy manifests as activity-related tendon pain with associated motor and sensory impairments. Tendon tissue changes in animals present in injured as well as contralateral non-injured tendon. This review investigated evidence for bilateral sensory and motor system involvement in unilateral tendinopathy in humans.
Methods A comprehensive search of electronic databases, and reference lists using keywords relating to bilateral outcomes in unilateral tendinopathy was undertaken. Study quality was rated with the Epidemiological Appraisal Instrument and meta-analyses carried out where appropriate. Analysis focused on comparison of measures in the non-symptomatic side of patients against pain-free controls.
Results The search revealed 5791 studies, of which 20 were included (117 detailed reviews, 25 met criteria). There were 17 studies of lateral epicondylalgia (LE) and one each for patellar, Achilles and rotator cuff tendinopathy. Studies of LE were available for meta-analysis revealing the following weighted pooled mean deficits: pressure pain thresholds (−144.3 kPa; 95% CI −169.2 to −119.2 p<0.001), heat pain thresholds (−1.2°C; 95% CI −2.1 to −0.2, p<0.001), cold pain thresholds (3.1°C; 95% CI 1.8 to 4.4, p<0.001) and reaction time (37.8 ms; 95% CI 24.8 to 50.7, p<0.001).
Discussion Deficits in sensory and motor systems present bilaterally in unilateral tendinopathy. This implies potential central nervous system involvement. This indicates that rehabilitation should consider the contralateral side of patients. Research of unilateral tendinopathy needs to consider comparison against pain-free controls in addition to the contralateral side to gain a complete understanding of sensory and motor features.
- Tendons
Statistics from Altmetric.com
Introduction
Tendinopathy impacts substantially on participation in physical activity1 and is characterised clinically, by activity-related pain, focal tenderness on palpation and decreased functional capacity of the segment (eg, strength and movement).2 Historically, tendinopathy has been considered as local degeneration with pathological changes including increased type III collagen fibres, an associated increase in ground substance and subsequent loss of hierarchical structure of the tendon.3 ,4 This loss of cellular homeostasis5 has been suggested to contribute to neovasularisation, which has been variously proposed to relate to features as diverse as tendon repair6 and chronic pain.7 Studies using an animal model of unilateral tendinopathy have confirmed local signs including; degenerative changes, neovascularisation8 and changes in the mechanical properties of the tissue including decreased elasticity and maximum stress at failure.9 This diverse array of changes is likely to affect the sensory and motor systems, yet there is limited understanding of how they are related.
An interesting and paradigm challenging observation from an animal model of repetitive unilateral exercise has been the presence of bilateral tendon changes, that is biological changes in the tendon of the non-exercised limb. This was evidenced by increased infiltrating macrophages not only in the tendon of the injured limb but also in the contralateral limb,10 a significant increase in tenocytes in both limbs11 and a bilateral increase in vascularity of the tendon by week 3. These observations lead to speculation of a centrally mediated process in the pathogenesis of tendinopathy, which underpins activity-related pain and disability, but this has received limited attention in literature.
The biological evidence of bilateral tendon pathology in a unilateral exercise-induced tendinopathy underpins the speculation that bilateral changes are likely to manifest in patients who present with a unilateral tendon problem and the pathogenesis of this condition may be more complex than is readily explained by local pathology. This systematic review aimed to address the issue of motor and sensory system changes associated with activity-related pain related to the tendon. To this end we systematically assessed the literature of human experimentation to ascertain whether changes in the motor or sensory systems occur in the contralateral side of patients with unilateral tendinopathy.
Methods
Search strategy
A comprehensive search of electronic databases (MEDLINE—via Ovid, Scopus and PubMed) was undertaken by LH to identify all English language studies for all years up to May 2013. Keyword, title and abstract information were used. Search terms were ‘tennis elbow AND bilat*’ (the symbol is used for identifying all words starting with bilat, eg, bilateral, bilaterally and bilateralism) OR jumper's knee AND bilat* OR ‘tendin* AND bilat*’ OR ‘tendo* AND bilat*’ OR ‘epicondy* AND bilat*’. A thorough manual search of the reference lists for all included studies was undertaken to identify articles that may not be listed on electronic databases, articles without abstracts that may have been missed by the initial search strategy, articles from networks or conferences and grey literature (ie, theses and books).
Study selection
Upon retrieval from the above search strategy all titles and abstracts were scanned by LH to identify studies that included bilateral measurement in patients with unilateral tendinopathy, and with a healthy cohort included for comparison. An a priori decision was made that a deficit on the side contralateral to the symptoms could be confirmed if the measure of sensory or motor function of the contralateral limb was different to that reported for the corresponding limb of control participants. Presence of bilateral deficits could not be determined from comparison between sides within a participant with unilateral symptoms as the absence of difference between sides could indicate that either (1) no deficit was present for either side or, (2) a deficit was present for both sides. Thus studies without a healthy control group for comparison could not be included.
For the purposes of this review, we defined the motor system broadly as encompassing bone, joint, tendon and muscle as well as neuromuscular control. The sensory system was defined as involving nociceptive and proprioceptive systems, usually measured with quantitative sensory testing.
All eligible studies were recorded and the full text was obtained. LH then undertook a detailed evaluation using predetermined criteria based on study design, clinical diagnosis of unilateral tendinopathy and quantitative reports of bilateral measures. Only data representative of unilateral tendinopathy were included in this review. Studies that included individuals with both bilateral and unilateral tendinopathies were retained if data were reported separately for the unilateral cases. Reviews, case studies, letters to the editor and studies of animals were excluded, along with non-English language publications.
Quality assessment
The quality of the included studies was scored using the epidemiological appraisal instrument (EAI).12 The EAI was condensed to 26 items. As this review was not focused on clinical trials, items related to randomisation, follow-up and environmental variables were not applicable and excluded from the assessment. Prior to the quality evaluation, detailed criteria to determine each response were modified from the original tool to match the purpose of this review and agreed on by all assessors. Two independent assessors scored the studies. Any disagreements were reviewed by consultation with a third party. Each item was independently scored using the standardised scale; ‘Yes’ (score=1), ‘Partial’ (score=0.5), ‘No’ (score=0), ‘Unable to determine’ (score=0) or ‘Not applicable’ (item was removed from scoring). Studies were given an overall score, which was derived as an average of the total for all 26 items (range 0–1).
Data extraction
LH completed data extraction, with all queries discussed and resolved by all assessors. Data describing the sample population and study methodology as well as the descriptives for the reported measures of pain, sensory and motor function were extracted for the contralateral side in unilateral tendinopathy and the corresponding side in controls. If additional information was required authors were contacted.
Studies were reviewed for measures of pain, sensory and motor functions. Measures were considered relevant if they measured any aspect of the sensory system (eg, pressure or temperature pain thresholds and proprioception), physical features of anatomy (eg, wrist angle and structural tendon changes) and motor function (eg, reaction time (simple and complex), corticomotor excitability, movement, muscle output (eg, grip strength)).
Statistical methods
The reliability of the quality assessment was evaluated using SPSS V.17 software (SPSS Inc, Chicago, Illinois, USA). κ Statistics were used to report the total inter-rater reliability between the two assessors. Inter-rater reliability was considered as poor (<0.00), slight (0.00–0.2), fair (0.21–0.4), moderate (0.41–0.6), substantial (0.61–0.8) or almost perfect (0.81–1.0).13 Where possible and appropriate the data were pooled with formal meta-analytical techniques using RevMan 5 (Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, 2006). A meta-analysis was performed using a random effects model to obtain weighted pooled mean differences and their 95% CIs. I2 was calculated and used as an indicator of the extent between trial heterogeneity. Differences in sensory and motor system measures between the side contralateral to the tendinopathy symptoms in patients and the corresponding side in pain-free control participants were calculated such that negative differences indicate that the measure for the patient with unilateral tendinopathy represented a deficit relative to that for the control participants, and positive differences indicate the opposite. Standardised mean differences (SMD) were calculated where meta-analysis was not possible. SMDs were interpreted as small 0.2, medium 0.5 and large 0.8 effect size.14
Results
Database search
The comprehensive search strategy yielded a total of 5791 publications from electronic databases and manually searched reference lists. All titles and abstracts were screened and 117 potentially relevant studies were identified. Of these, 25 satisfied the selection criteria and reported bilateral nociceptive, sensory and motor measures of participants with unilateral tendinopathy contrasted with data for controls (figure 1). Two studies were excluded as they reported secondary presentation of data published elsewhere.15 ,16 Seven authors were contacted during data extraction to provide additional information for the following reasons: data only presented graphically17; affected and unaffected limb data combined18–20; no control data for a specific outcome measure21 and insufficient details for data.22 ,23 Three authors supplied data on at least one outcome; one provided insufficient useable data; and two were unable to be contacted. Of the 25 studies that satisfied the inclusion criteria a total of 20 were included in the review. The composition of these per anatomical region included 17 LE, 1 patella tendinopathy, 1 Achilles tendinopathy and 1 rotator cuff tendinopathy.

Selection process for inclusion in the review.
Study characteristics
Studies varied in terms of location, timing and population. Eight studies (40%) were conducted in Australia, four (20%) in Spain, two (10%) in Canada and one (5%) each in the USA, the UK, Finland, Norway, Sweden and Denmark. One study (5%) was published in the 1980s; two (10%) in 1990s; 11 (55%) in 2000s and six (30%) since 2010. Sample sizes varied widely from 1924 to 238 participants.25 In general the number of LE participants did not match the number of controls.
Quality assessment
The overall agreement between the two reviewers was almost perfect (κ=0.897, p<0.01)13 with 484 agreements of 520 decisions. The results from the quality assessment using the modified EAI12 demonstrated a median score of 0.46 (range 0.29–0.63) out of a possible 1 (quality assessment results, web only supplementary file A). Overall the quality assessment revealed only 15% (3 of 20) used diagnostic imaging as part of the eligibility criteria; only 25% (5/20) clearly described their study population and how and where they recruited participants, and only 20% (4/20) used priori sample size calculations. Only 35% (7/20) of the studies described their study design and no longitudinal or prospective studies were identified. The two reviewers were unable to determine if any study blinded the participants to the outcome measures and only 15% (3/20) of studies blinded the assessors to the participant's condition during the experiments. Despite the importance of using validated measures only 5% (1/20) of the studies reported the validity of their main measures. No studies included prior history of the condition in the analysis, 20% (4/20) adjusted for individual covariates and confounders, 10% (2/20) reported the results by severity of the condition and 15% (3/20) reported the results by subgroups defined by age and gender.
Meta-analysis
Not all studies contributed data to the meta-analysis as many were the only study for tendinopathy in a specific anatomical location (ie, patella tendinopathy, rotator cuff tendinopathy and Achilles tendinopathy) and there were differences in measurements used, with some reported in only one study (eg, corticomotor excitability or electrical pain thresholds). The studies that could not be included in the meta-analysis are discussed individually in the ‘appraisal’ section. Only studies of patients with LE could be subjected to meta-analyses. Of these, six studied pressure pain threshold at sites other than the elbow, three studied heat pain and cold pain thresholds bilaterally, and two studied reaction time and speed of movement bilaterally.
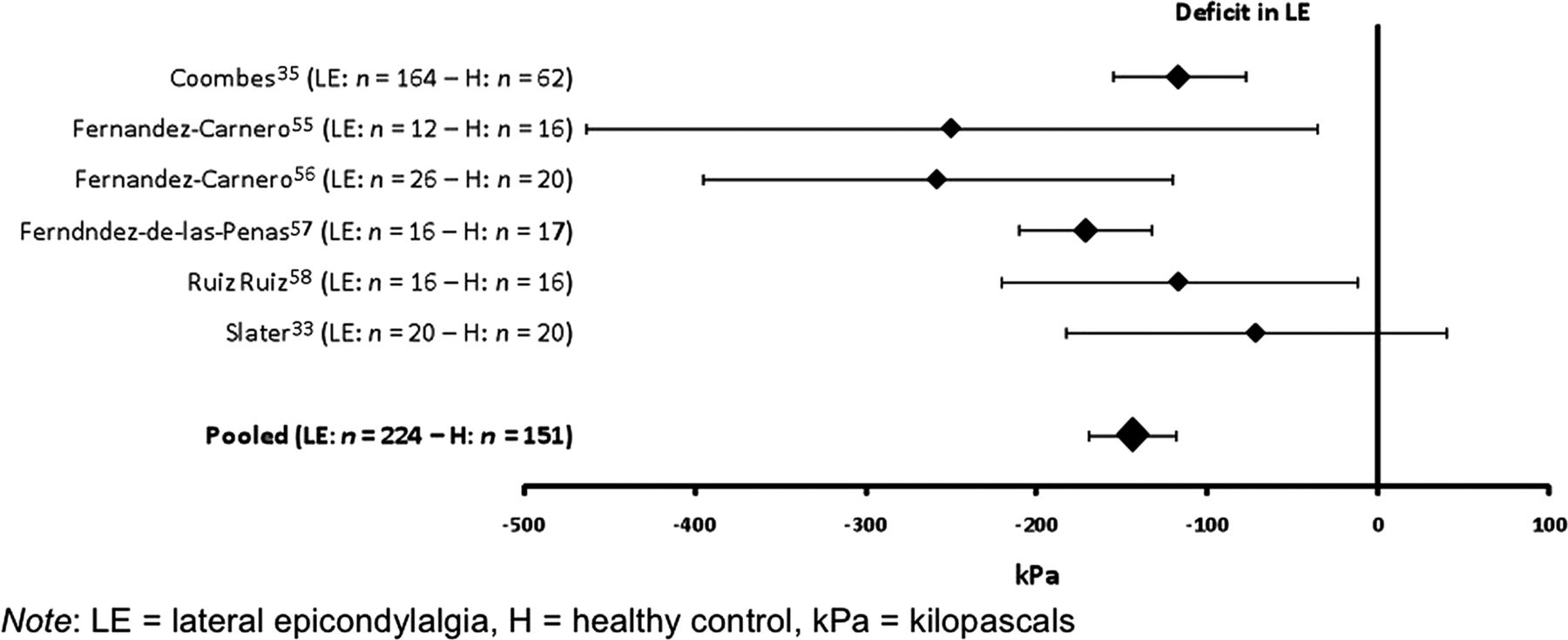
The weighted pooled mean difference demonstrated that pressure pain thresholds were 144.3 kPa (95% CI 119.2 to 169.2, I2=46%) lower in the participant's limb that was contralateral to the unilateral LE symptoms than the corresponding side of controls (p<0.001; figure 2). Heat pain thresholds were 1.2°C (95% CI 0.2 to 2.1, I2=33%) lower and cold pain thresholds were 3.1°C (95% CI 1.8 to 4.4, I2=0%) higher on the contralateral side of participants with unilateral LE than the corresponding side of controls (p<0.001; figure 3).

Forest plot for pressure pain thresholds.
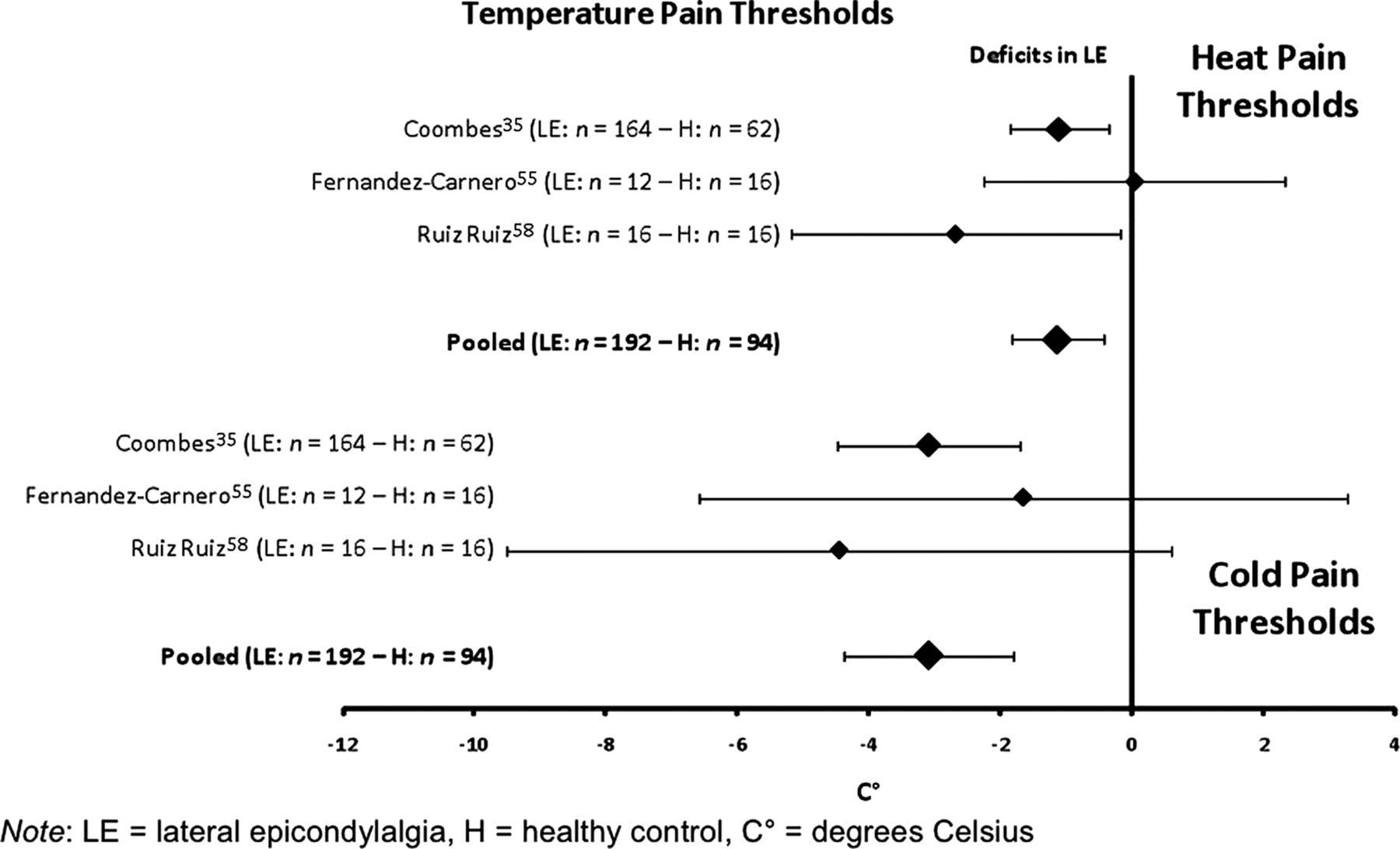
Forest plot for temperature pain thresholds.
Reaction time to lift the hand off a button task was 37.8 ms (95% CI 24.8 to 50.7, I2=54%) slower and two choice reaction time in a movement to a target task was 36.0 ms (95% CI 25.8 to 46.1, I2=0%) slower in the contralateral side of patients than the corresponding side of controls (p<0.001; figure 4). Speed of movement was 20 cm/s (95% CI 35.3 to 4.6, I2=52%) slower in the contralateral side of patients than controls (p<0.001; figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for reaction time and speed of movement.
Appraisal
Studies unable to be included in the meta-analysis are considered in four key themes related to changes in (1) motor, (2) sensory and (3) nociceptive systems, as well as (4) variants in anthropometry/anatomy. This section presents differences between the contralateral limb of patients and data for control participants (SMD and 95% CI of all included studies, web only supplementary file B). All included studies of sensory, motor and nociceptive systems and the majority of the muscle strength studies investigated unilateral LE.
Motor measures
A study of corticomotor excitability (resting motor threshold, stimulus response curve, silent period and motor evoked potential), as measured by transcranial magnetic stimulation, demonstrated no differences between the affected or contralateral limb in 14 patients and 16 controls.26 Electromechanical delay during gripping (n=13 patients and controls)27 is longer in patients’ contralateral side (mean: 64±24 ms) compared with controls (mean: 39±14 ms; p<0.001), while rate of force development (in the same study) did not differ between the two groups. Evaluation of wrist position during a spontaneous gripping task in 40 patients and 40 controls showed patients gripped in 11° (95% CI 7° to 14°, p<0.001) more flexion than controls, bilaterally.23 Two studies assessed one-choice reaction time of pointing to a target and speed-of-movement in patients compared to controls,25 ,28 which could not be meta-analysed due to significant heterogeneity, I²=76% (p<0.001). Both demonstrated slower reaction time on the contralateral side of the patients than the controls (13% (SMD 0.84) and 22% (SMD 1.13)).25 ,28
Five studies investigated maximal grip strength, using a hand-held dynamometer, in patients with unilateral LE,23 ,27 ,29–31 which could not be meta-analysed due to significant heterogeneity I²=89% (p<0.001). Three demonstrated a small (SMD 0.24 to 0.36),27 ,29 ,30 and one a large (SMD 2.38) reduction in strength in patients than controls.31 The remaining study demonstrated a greater strength (SMD −0.59) in patients (284±79N) than controls (mean 234 N±86).23 All studies, except one31 demonstrated a significant difference between sides within the patient group.23 ,27 ,29 ,30
Studies of other strength measures have focused on upper limb tendinopathy, particularly unilateral LE. Isometric elbow flexion and extension strength has been shown to be no different between 164 patients with unilateral LE and 54 controls32 (patients—flexion; 246.7±40.4 N, extension 185.9±31.8 N; controls—flexion; 245.7±40.4 N, extension; 185.9±32.3 N; SMD Flexion 0.02, SMD Extension 0.00). Wrist extension strength has been shown to be 24% less in 20 patients (87.0±40.3 N) than controls (114.0±30.3 N; SMD 0.75).30 Another study reported isometric strength measures of a range of upper limb muscles in 16 patients with unilateral LE and controls and showed a strength deficit of 16–29% (table 1).31 There was no significant difference between sides in the patients for any of the strength measures (p=>0.05).
Strength measures between the contralateral side of patient and healthy controls (mean±SD)
Isometric strength has also been assessed for unilateral rotator cuff tendinopathy. Rather than a decrease, isometric shoulder abduction strength was 15% greater in 10 patients with unilateral rotator cuff tendinopathy compared with 9 controls24 (patients: 223±89 N; controls: 189±63 N, SMD 0.44).
Sensory measures
Proprioceptive acuity has been assessed by the ability to discriminate between two weights between 100 and 130 g in steps of 2 g increments using custom-built equipment.26 Weber's fraction, which expresses the acuity threshold (minimum difference in weight that can be detected) as a proportion of 100 g, was not different between the contralateral side of patients and controls (4.9±3.2%; and 5.4±2.1%, respectively, p>0.05),33 but was less for the affected side (8.2±3.0%, p=0.001) than the contralateral side.
Nociceptive system measures
In contrast to the meta-analysis for pressure and temperature pain thresholds, a study of electrical pain thresholds by means of stimulation to the skin over extensor carpi radialis, in 18 patients and 16 controls, demonstrated no significant difference between the contralateral side of the patients and controls,34 but the affected side was significantly more sensitive than the contralateral side.
Muscle trigger points have been assessed using a standardised method by an experienced assessor blind to the patient's condition, in 25 patients and 20 controls.21 The number of latent trigger points in the contralateral side of patients (2.2, 95% CI 1.8 to 2.6) was higher than that in controls (0.4, 95% CI 0.0 to 0.07, p<0.001, SMD 0.89).
Anatomic/anthropometric measures
In patients with patella tendinopathy,18 longitudinal arch height of the foot, during maximum weight bearing is lower in patients (42.0±7.4 mm) than controls (50.4±5.9 mm; SMD 1.29), but there were no differences between sides within the patient group (affected: 42.3±8.2 mm). There was no difference in an indirect measure of hamstring length or ankle dorsiflexion between groups.
Two imaging studies used ultrasound to measure local anatomy at the Achilles tendon (in unilateral mid-portion Achilles tendinopathy)35 and the common extensor tendon of the elbow (in LE),20 without blinding of the sonographer. The thickness of the Achilles tendon was slightly greater and the echogenicity less on the contralateral side of 11 patients with Achilles tendinopathy (6.6±1.2 mm and 82.9±12.9 U, respectively) than that of 9 controls (5.0±1.3 mm and 119.3±13.5 U, respectively; p=<0.05).35 The affected tendon (9.4±1.2 mm) was thicker than the contralateral tendon, but there was no difference in echogenicity (76.7±11.7 U). Another study investigated the accuracy of power Doppler imaging for the diagnosis of unilateral LE.20 There was a tendency towards a thicker tendon on the contralateral side of patients (n=18) than controls (n=19), which was in the order of 0.50 mm (95% CI 0.00 to 0.99, p=0.05) or 11% of the control group mean tendon thickness (4.47 mm). This difference was comparable to the 15% greater thickness of the affected tendon (mean—5.82 mm; difference—0.86 mm (95% CI −1.35 to −0.36; p=0.002) than the unaffected tendon in the LE group.
Discussion
This review provides a synthesis of research findings of sensory and motor differences, compared with pain-free controls, in the limb contralateral to the side of symptoms in patients with unilateral tendinopathy. In general, meta-analysis of data from multiple studies provides evidence of significant deficits in the sensory and motor systems, including pressure and thermal pain thresholds, simple reaction time, two-choice reaction time and speed of movement. These results align with findings from other studies that could not be included in the meta-analyses (due to study population or measurements) and studies of other musculoskeletal conditions that demonstrate contralateral sensory and motor system deficits in patients with unilateral carpal tunnel syndrome,36 and chronic wrist pain.37 For instance, Fernandez-de-las-Penas36 reported lower pressure pain thresholds over the peripheral nerves, the carpal tunnel and the C5–C6 zygapophyseal joints of the non-affected side in women with unilateral carpal tunnel syndrome than for pain-free controls. Smeulders37 quantified motor control using a writing task with measures of fluency, size and velocity of stroke patterns in patients with unilateral chronic wrist pain and controls. The patients were significantly less fluent than the controls in both their affected and contralateral arm, suggesting bilateral motor system deficits.
It is tempting to speculate that sensory system deficits might be attributed to abnormalities of central pain processing. Central sensitisation arises from convergence of noxious and non-noxious inputs on the wide dynamic range neurons in the dorsal horn38 with subsequent enhanced sensitivity to painful (hyperalgesia) and normally non-painful (allodynia) stimuli over an area extending beyond the injured segment. Central sensitisation is present in many chronic pain conditions such as fibromyalgia, low back pain, complex regional pain syndrome,39 migraine, tension-type headache and myofascial pain syndrome.38 The widespread hyperalgesia extending to the contralateral limb in unilateral tendinopathy appears similar to that present in other chronic pain states.
Several mechanisms may explain the bilateral changes in motor system function. First, it is well known that unilateral exercise leads to strength and skill adaptations bilaterally through a process known as ‘cross education’.40 Significant gains in contralateral strength41 ,42 and skill43 have been shown with unilateral exercise, regardless of whether it is active volitional, facilitated (electrical stimulation) or imagined. The reverse, due to a unilateral reduction in activity might explain the effects in the contralateral side. The underlying mechanisms for cross education are poorly understood, but likely involve spinal and supra-spinal centres. As H-reflex amplitudes (which largely depend on spinal motoneuron excitability) do not change in the untrained muscle, despite strength gain44–46 supra-spinal mechanisms are more likely. Relevant cortical mechanisms are thought to involve a complex network of interhemispheric connections and ipsilateral corticospinal fibres from the primary motor cortex, which provide neural drive to the contralateral muscle during unilateral contraction.47 ,48 Corticospinal excitability (measured by transcranial magnetic stimulation) to hand muscles increase during contraction of the opposite side,49–51 which implies interhemispheric interactions. Functional MRI (fMRI) has demonstrated that changes in activation of the contralateral motor areas (premotor and primary motor cortex) are similar in both sides during unilateral activation,52–54 and unilateral exercise elicits activation in the contralateral somatosensory54 and left temporal cortices (involved in movement memory).52 This finding suggests that the somatosensory cortex may play a pivotal role in bilateral strength gains with unilateral training. It remains unknown, but possible that deconditioning of the affected limb in unilateral tendinopathy exhibits a negative form of cross education. This requires further investigation. Second, an alternative explanation for the bilateral motor changes is that these features were different from the healthy controls in these individuals prior to the onset of tendinopathy and the motor differences could even contribute to the condition's development. This requires consideration in longitudinal studies.
The studies excluded from the meta-analysis demonstrated consistent lower grip strength on the contralateral side of patients with unilateral LE than controls in four of five studies23 ,27 ,29 ,30 and medium-to-large strength deficits at other distal and proximal joints of the upper limb.30 ,31 There were no differences for the direct comparison of elbow flexion and extension between the contralateral side of patients and the controls.32
Two studies revealed a substantial increase in strength of the contralateral side of patients compared with controls.23 ,24 One demonstrated increased grip strength on the contralateral side of patients with unilateral LE (SMD −0.59),23 whereas the other demonstrated increased shoulder abduction strength in patients with unilateral rotator cuff tendinosis (SMD −0.44).24 There are several possible explanations. First, it is possible that the augmented strength is secondary to a compensatory increase in the functional use of the unaffected side to protect the injured limb. Second, the patient group might have been stronger than the controls prior to the development of the unilateral tendinopathy as a result of activity, which may underpin the increased use of the limb leading to the tendinopathy.23 Both scenarios could be addressed by the adoption of a prospective longitudinal study design.
Bilateral sensory and motor system deficits in unilateral tendinopathy require consideration in both clinical practice and research for several reasons. First, the findings of this review highlight the importance of inclusion of a healthy matched control group for comparison in studies of features of tendinopathy. Second, the presence of differences relative to controls on both the symptomatic and non-symptomatic sides suggests that there could be benefit from rehabilitation that addresses motor and sensory system features on both sides. Specific training of the contralateral limb may also provide additional benefits to the affected limb through cross education, through the mechanism discussed above. Third, patients participating in sports or occupations requiring rapid bilateral reaction time and movement speed such as trap shooting and boxing, may require specifically targeted training to address deficits that may present bilaterally.
This review has some limitations, which require consideration. The meta-analyses included only a small number of studies with small sample sizes and of only one tendinopathy (ie, LE). There is a clear need for additional studies with larger sample sizes across a range of tendinopathies. The quality of studies varied substantially and was overall quite low. A key limitation was the lack of confirmation of localised tendinopathy using diagnostic imaging. Only two studies required confirmation of pathology with diagnostic imaging for inclusion into the study, and even then neither reported the measure's reliability and only one used diagnostic imaging to verify healthy tendon in controls.
In conclusion this review highlights that sensory and motor system deficits are common in the non-injured limb of patients with unilateral tendinopathy, particularly in LE, which has received most attention in literature. These data suggest involvement of the central nervous system in sensory and motor deficits seen in unilateral tendinopathy, which likely contribute to the expression of pain and disability. The results clearly demonstrate that the contralateral side of the body cannot be used as a reference standard for assessment, either in clinical practice or research and that treatments other than those that target local pathology are likely to be required.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online appendix
Footnotes
-
Contributors LH, PH and BV contributed to conception, design and construct of the study. LH, EL and BV conducted the comprehensive search, critical appraisal and analyses. All authors contributed to manuscript writing. BV and LH are guarantors of the overall content.
-
Funding Funding was provided by a Programme Grant (NHMRC Program Grant #631717) and Research Fellowship (PH) from the National Health and Medical Research Council of Australia and an Australian Postgraduate Award scholarship (LH).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.