Article Text

Abstract
Objective To compare the efficacy of different injection therapies for plantar fasciopathy (historically known as ‘plantar fasciitis’).
Design Systematic review and network meta-analysis.
Data sources Electronic databases (MEDLINE, CENTRAL, Web of Science and Scopus) were searched up to 11 July 2015 for completed studies.
Eligibility criteria for selecting studies We considered randomised trials comparing various injection therapies in adults with plantar fasciopathy. The primary outcome was pain relief. Secondary outcomes included functional disability, composite and health-related outcomes. All outcomes were assessed (1) in the short term (up to 2 months), (2) the intermediate term (2–6 months) and (3) the medium term (more than 6 months to 2 years). Quality assessment was performed using the Cochrane risk of bias tool.
Results We included 22 trials comprising 1216 patients. Dehydrated amniotic membrane injections were significantly superior to corticosteroids in the short term in achieving the primary and composite outcomes (mean difference (MD) in visual analogue scale (VAS) was −7.32, 95% CIs −11.2 to −3.38; and MD in the foot health status questionnaire was 31.2, 95% CIs 13.9 to 48.6, respectively). For pain relief, botulinum toxin-A provided a significant short-term advantage over placebo, which was still present at 6 months (MD in VAS was −2.9, 95% CIs −4.44 to −1.39; and MD −4.34, 95% CIs −7.18 to −1.54, respectively).
Summary Although the dehydrated amniotic membrane provided significant clinical relief at 0–2 months, there were no data about this treatment at 2 months and beyond. Botulinum toxin-A injections significantly reduced pain intensity at 0–6 months.
Systematic review registration number CRD42015017353.
- Meta-analysis
- Intervention efficacy
- Rehabilitation
- Foot
Statistics from Altmetric.com
Introduction
Plantar fasciopathy (PF) is one of the most common causes of foot pain in adults.1 The prevalence of PF in the general population varies between 3% and 7%,2 ,3 and accounts for 8% of injuries in studies of runners.4 ,5 The peak incidence of PF occurs between 40 and 60 years of age.6 Although PF may be a self-limiting condition,7 ,8 it impairs health-related quality of life,9 and the economic burden to the US healthcare system in 2007 alone was estimated at between $192 and $376 million.10
The first-line treatment options for PF include:11 weight loss, activity limitation, avoidance of barefoot walking and flat shoes, heel cups and arch support, home cryotherapy, stretching exercises, padding and strapping of the foot, orthotic insoles, oral anti-inflammatory drugs and corticosteroids injections. The following options may be considered as second-line treatments: continuation of the initial therapy, prefabricated and custom orthotic devices, night splints, corticosteroid injections, other injection therapies (eg, botulinum toxin-A (BTX-A) intervention), physical therapy and cast or boot immobilisation. If symptoms persist for more than 6 months, Extracorporeal Shock Wave Therapy (ESWT) treatment and surgical consultation are suggested as third-line treatment options.11
Currently, more than 10 different injectable treatments are available for the management of PF. The aim of our systematic review and network meta-analysis was to compare the therapeutic efficacy of various injection therapies in adults with PF.
Methods
Protocol and registration
We prospectively registered this systematic review and network meta-analysis with PROSPERO (CRD42015017353) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for Network Meta-Analyses.12
Eligibility criteria
We included randomised controlled trials (RCTs) that compared the effects of at least two different injectable treatments for PF. We considered both the two-arm parallel group and multiarm trial designs. Adult patients who suffered from PF were eligible for inclusion in this systematic review and network meta-analysis. Participants were treated with wet needling, dry needling or both. We excluded animal studies and patients with full-thickness fascia tears.
Information sources and search
We searched the following electronic databases for completed published and unpublished studies up to 11 July 2015: MEDLINE, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science and Scopus. The following clinical trial registries were searched: International Standard Randomised Controlled Trial Number (ISRCTN) Register, ClinicalTrials.gov and the Australian New Zealand Clinical Trials Registry (ANZCTR). We also examined reference lists of relevant systematic review articles for additional completed studies.
The search strategy for MEDLINE is presented in online supplementary file 1. We adapted this strategy to each included electronic database. We applied neither specific database filters nor language restrictions to our database searches.
Supplementary file 1
Study selection
Two authors (KT and HV) independently searched the literature for potentially relevant articles through electronic database and manual search. After the removal of duplicates, we screened the titles and abstracts of the retrieved records for eligibility. Then, the full text of the remaining articles was screened for further consideration. In case there was insufficient information for quantitative synthesis in an included RCT, we contacted the corresponding author of the trial twice to request additional information. If the corresponding author did not respond to this request, we excluded the RCT from the quantitative synthesis. Any discrepancies about the study selection process were resolved by KT and HV in discussion.
Data extraction
Data extraction was independently performed by two reviewers (KT and HV), and included the following elements: year of publication, countries in which the RCTs were conducted, number of the enrolled and analysed patients, number of completers, patient demographics, diagnosis confirmation, duration of symptoms, comparators in the intervention groups, image guidance of the intervention, intervention characteristics and postrehabilitation exercises. It also included information about the risk of bias assessment, outcome measures, previous treatments and side effects. In cases with missing information, the study authors were contacted to request their data.
If there was more than one clinical condition under treatment in an included RCT, we abstracted information only about patients suffering from PF.
Risk of bias assessment
Two investigators (KT and HV) independently assessed the quality of individual trials using the Cochrane risk of bias tool.13 The following domains were considered: sequence generation, allocation concealment, blinding of patients, masking of personnel and blinding of outcome assessors, incomplete outcome data, selective reporting and ‘other bias’. Each entry was classified to be at a low, unclear or high risk of bias.
We also assessed the risk of bias across trials. If more than 50% of the information was from trials at a low risk of bias, the domain was judged to be at a low risk of bias. Similarly, if most information was from RCTs at an unclear/high risk of bias, the domain was considered to be at an unclear/high risk of bias.
We used a preplanned multiple (stratified) analysis strategy for the incorporation of the risk of bias assessment into the results of this systematic review and network meta-analysis.13 This strategy included an analysis with and without studies at an unclear/high risk of bias according to the components of sequence generation and masking of the participants.
Outcomes
The primary outcome of this study was pain relief, pain intensity or both. We selected this main outcome as our primary outcome because pain is the predominant symptom in patients with PF. Therefore, we expected that pain intensity would be more comprehensively analysed in the identified RCTs compared to other outcomes. We assessed the primary outcome either by instruments (in forms of questionnaires) that measure pain intensity or by subscales of composite instruments (eg, Foot Health Status Questionnaire (FHSQ) pain subscale).
Secondary outcomes included functional ability, disability or both. We measured this outcome using subscales of composite instruments which assess functional ability, disability or both. Secondary outcomes also included composite outcomes, measured by instruments that assessed functional disability and pain intensity as a minimum. In addition, we included health-related outcomes, measured using subscales of relevant questionnaires. Finally, we reported side effects using the broad focus approach described in the Cochrane Handbook.14 We also classified unintended effects into minor and major.
We accounted for all the scales and subscales of different instruments that assessed the same outcome in an included RCT, with the aim of increasing homogeneity in terms of the outcomes of this network meta-analysis.
For all study outcomes, there were three follow-up periods of assessment:
Short term: up to 2 months after treatment.
Intermediate term: 2–6 months after treatment.
Medium term: more than 6 months to 2 years after treatment.
Statistical analysis
In this study, we performed two types of meta-analyses. For all study outcomes, we conducted pairwise meta-analyses to get the direct estimates for each included comparison. Then we proceeded with network meta-analysis to get the network estimates.
Network meta-analysis synthesises both direct and indirect estimates. It provides estimates for the relative efficacy of treatments, even if they have never been directly compared in head-to-head trials.15–17 Another important outcome is that network meta-analysis allows a ranking of competing interventions.
Pairwise meta-analysis
We conducted pairwise meta-analysis of change-from-baseline scores using the Review Manager software18 and a random-effects model.19 We tested heterogeneity with the Q statistic, and a p value of less than 0.05 indicated statistical significance. We also measured the extent of heterogeneity with the I2 statistic.20 For all study outcomes, we performed the analyses on the basis of standardised mean differences (SMDs) with 95% CIs.
Network meta-analysis
We used STATA software (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP) to perform network meta-analysis with the mvmeta command and routines presented in Chaimani et al.21 A p value of less than 0.05 was judged to be statistically significant. We reported results as SMDs with 95% CIs.
We conducted network meta-analysis of change scores using a random effects statistical model. If there were missing change-from-baseline SDs in an included trial, we imputed them according to Cochrane guidelines.22 In these imputations, we assumed a correlation coefficient of r=0.5 between the baseline and follow-up measurements. If an enrolled RCT did not report SDs for a study outcome, we borrowed SDs from another study of this meta-analysis, provided that this outcome was assessed with the same instrument(s).23 If there was more than one trial assessing this outcome with the same instrument(s), we borrowed the largest SDs.
Graphical tools in the network meta-analysis
We visually represented the networks of interventions in network meta-analysis plots. In these plots, head-to-head comparisons were shown by edges. The thickness of edges was proportional to the number of studies for each comparison, and the size of nodes was proportional to the number of participants randomly assigned to each intervention. If the networks of interventions included more than 10 RCTs, comparison-adjusted funnel plots were created to assess the presence of small study effects.24 This was the case for the short-term and intermediate-term assessment of pain relief, and for the short-term assessment of composite outcomes.
We also calculated percentage contributions of each estimate in the networks of this review.25 In addition, we used Surface Under the Cumulative RAnking (SUCRA) probabilities to rank the efficacy of the competing treatments.26 SUCRA would be 1 if a therapy is certain to be the best and 0 if a therapy is certain to be the worst. SUCRA values show the percentage of effectiveness an intervention achieves with relation to an intervention that is always the best without uncertainty. We graphically represented the results of the ranking probabilities with their uncertainty with ranking probability plots.24–26 Finally, we created inconsistency plots to present the inconsistency factor (IF) with its CIs for each loop.
Transitivity
A key assumption of network meta-analysis is that of transitivity.27 Transitivity implies that the distribution of effect modifiers is similar across treatment comparisons. We explored transitivity through inspection of the characteristics of the included RCTs. We also explored it statistically by quantifying the differences between direct and indirect evidence in each closed loop of evidence. We also used the ‘design-by-treatment’ model.28 It is noted that in cases with star-shaped networks, inconsistency was untestable.24
Unit-of-analysis issues
We handled unit-of-analysis issues according to Cochrane guidelines.29 As for the incorporation of information from cross-over trials into this network meta-analysis, we considered only data from the first phase of interventions in the analyses.22 We combined the multiple intervention groups from an included RCT, provided that these groups compared the same injectable treatment in combination with a different co-intervention.22 ,30 As for the issue of repeated measurements on patients, we defined three different time frames assessment (ie, short-term, intermediate-term and medium-term follow-up). If there was more than one observation for the same outcome in the included RCTs, we considered the longest follow-up measurement per time frame.
Intervention arms in the network meta-analysis
We considered the following arms in this network meta-analysis: Corticosteroids (CSs), BTX-A, Autologous Whole Blood (AWB), placebo, Platelet-Rich Plasma (PRP), Non-steroidal Anti-Inflammatory Drugs (NSAIDs), Cryopreserved-human Amniotic Membrane (c-hAM), micronised Dehydrated Human Amniotic/Chorionic Membrane (mDHACM), Dextrose Prolotherapy (DP), Sham Dry Needling (SDN) and Polydeoxyribonucleotide (PDRN). The placebo arm contained one or more of the following comparators: normal saline, local anaesthetic, dry needling and tibial nerve block.
Clinical interpretation of the results
We used Cohen's rule of thumb for interpreting effect sizes.31 Thus, an SMD value of 0.2 showed a small effect, a value of 0.5 demonstrated a moderate effect, and a value of 0.8 indicated a large effect.
For pain relief, we re-expressed SMDs to mean differences (MDs) in VAS. We performed this back-transformation by multiplying SMDs with the median baseline SD of 2.4 in VAS, reported in a large-scale RCT in PF.32 ,33 Then we accounted for the direction of VAS by multiplying the MDs with −1.29 We thereafter used the Minimum Clinically Important Difference (MCID)34 of −9 mm for VAS for the clinical interpretation of mean change scores.35
For the secondary outcomes, we re-expressed SMDs to MDs in FHSQ scores and subscores. For these back-transformations, we borrowed the largest median baseline SDs reported in trials of the present systematic review. In contrast to VAS, higher scores in the FHSQ questionnaire represent improved patient-reported outcomes (PROs) (range 0–100). It is noted that the FHSQ questionnaire is one of the strongly recommended instruments for the clinical evaluation of patients with PF.36 For functional disability and health-related outcomes, we used the Minimum Clinically Important Differences (MCIDs) of 7 and 9 points for the FHSQ function and general foot health subscales, respectively.35 For composite outcomes, we imputed the MCID for the FHSQ scale, which was found to be 10.2 points. In this imputation, we accounted for the weighted MCIDs that we used for the FHSQ subscales.
Additional analyses
We followed a Bayesian Markov chain Monte Carlo approach using WinBUGS software37 ,38 to perform random effects meta-regression39 and subgroup analyses. The former was undertaken in networks with sufficient studies.29 The latter was linked to patients' demographics and different comparators in the placebo group. We considered the following effect modifiers in meta-regression: co-interventions, image guidance of the injections and duration of symptoms before the intervention.
Furthermore, we performed multiple a priori defined sensitivity analyses to investigate the impact of the imputed SDs on the results. We also undertook sensitivity analyses to explore the effects of various intervention characteristics, postrehabilitation exercises, previous treatments and confirmation of the diagnosis.
Finally, we conducted two sensitivity analyses to investigate the impact of the risk of bias on the results. In the first one, we excluded trials at an unclear risk of bias that explored the efficacy of PRP. The second one was a part of our predefined stratified analysis (ie, secondary analysis). In the latter sensitivity analysis, we excluded trials at a high or unclear risk of bias according to the elements of randomisation and masking of the participants.
Sensitivity analysis in a network meta-analysis
In a network meta-analysis, sensitivity analysis is performed by excluding the data of one or more trials from the analysis to investigate the impact of an effect modifier on the results of the quantitative synthesis.
Results
The literature search yielded 1137 potentially relevant records. We removed the duplicates and screened the remaining 744 articles for eligibility. Then we assessed the full text of 36 articles for inclusion. Three of these articles referred to non-randomised trials40–42 and two of them were letters to the editor.43 ,44 One study reported the results of the same trial at a different follow-up measurement.45 Six records referred to duplicates of published trials (ACTRN12610000239066, ACTRN12610000611022, NCT00447876, NCT01659827, ISRCTN36539116, and ISRCTN79628180). There were no available results for two trials (ACTRN12610000899044 and ISRCTN86484960).
At the end of the article selection process, we included 22 trials in the qualitative synthesis. Pooling was possible for 21 RCTs of this systematic review. The results of the screening and study selection procedure are presented in the flow chart of the present study (figure 1).
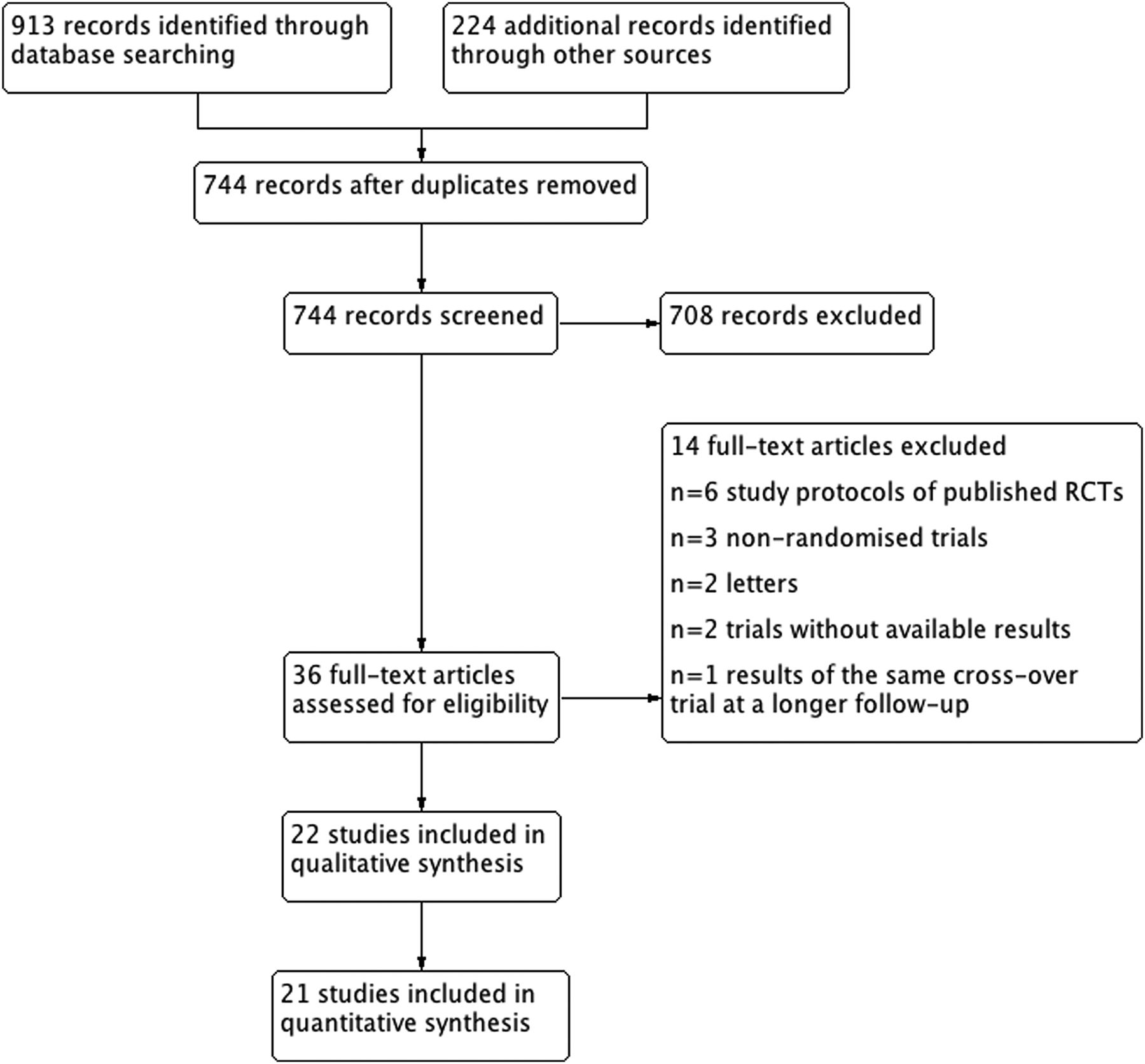
Flow chart of the study selection process. RCT, randomised controlled trial.
Study characteristics
The 22 RCTs provided 1216 participants for analysis. We abstracted information for 1197 patients. The number of participants who completed the follow-up measurements was 1107. The enrolled trials were published between 1999 and 2015. Furthermore, the diagnosis was confirmed with ultrasound (US) in three studies.46–48 In RCTs with available information, the mean ages of the participants ranged between 37 and 57 years. MRI was used to confirm the diagnosis in one trial.49 Two of the included trials were financially supported by research foundations,46 ,50 one by research campaign51 and four by industry.52–55 In line with the current form of the Cochrane risk of bias tool, we did not include funding in the quality assessment of the trials. Eight RCTs were conducted in Asia,47 ,48 ,54 ,56–60 five in Europe,51 ,55 ,61–63 five in America,49 ,52 ,53 ,64 ,65 two in Africa66 ,67 and two in Australia.46 ,50 The registration protocols were available for six studies in this review.46 ,50–52 ,55 ,62 It is noted that the longest follow-up observation in the included RCTs was performed at 96 weeks after treatment.49 The study characteristics are shown in online supplementary file 2a.
Supplementary file 2a
Ten of the 22 RCTs in this systematic review were placebo-controlled, whereas the rest were comparative trials. Real dry needling was used as a combination treatment in three studies of this systematic review.47 ,58 ,60 The SDN intervention included the use of non-penetrating sham acupuncture needles.68 The gauge of the needle that was used in the enrolled trials varied from 18 to 27 in cases with available data. The intervention characteristics are presented in online supplementary file 2b.
Supplementary file 2b
Risk of bias assessment
The results of the quality assessment of individual trials are presented in online supplementary file 3. The allocation was adequately generated in 15 trials and the risk of bias in the domain of randomisation was judged to be low. The participants and outcome assessors were successfully blinded in most trials (n=15, 68%; and n=14, 64%, respectively) and the risk of bias in these domains was judged to be low. As for the incomplete outcome data element, there was a low risk of bias because most information stemmed from studies at a low risk of bias (n=15, 68%). It is noted that there was no significant imbalance in the baseline characteristics in most RCTs (n=19, 86%).
Supplementary file 3
There was a high risk of bias in the blinding of personnel's domain because the proportion of studies at a high risk of bias in this component was sufficient enough to affect the results. We considered that the risk of bias was unclear for the domain of allocation concealment because there was insufficient information about the methods used to conceal the allocation in half of the studies (n=11). Moreover, there was an unclear risk of selective outcome reporting because more than 50% of the studies were at an unclear risk of bias in this domain (n=14, 64%). The quantification of the risk of bias assessment is presented in figure 2.
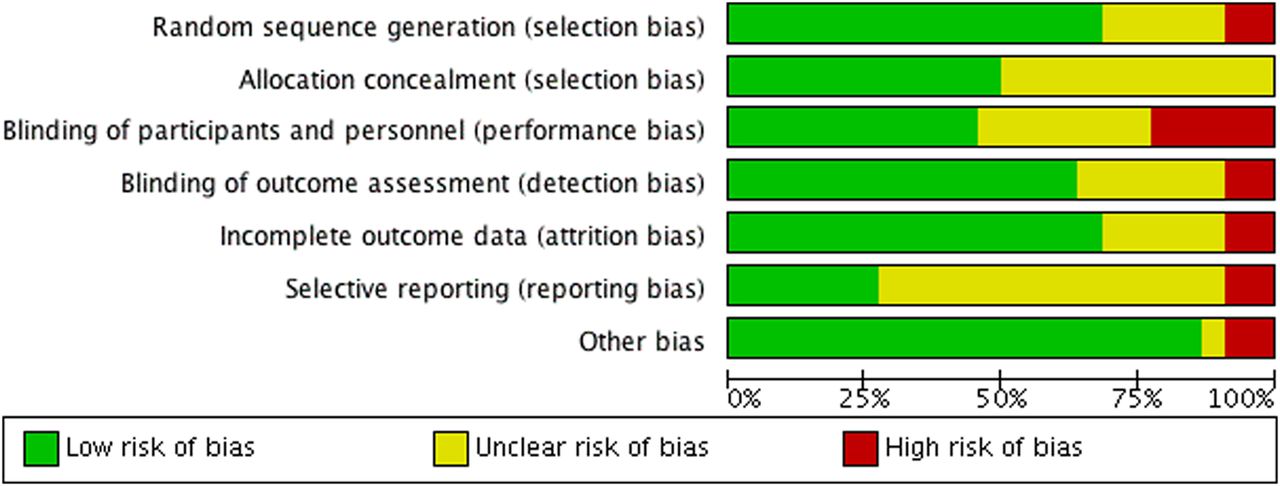
Quantification of the risk of bias assessment.
Synthesis of the results
Short-term outcome assessment (0–2 months)
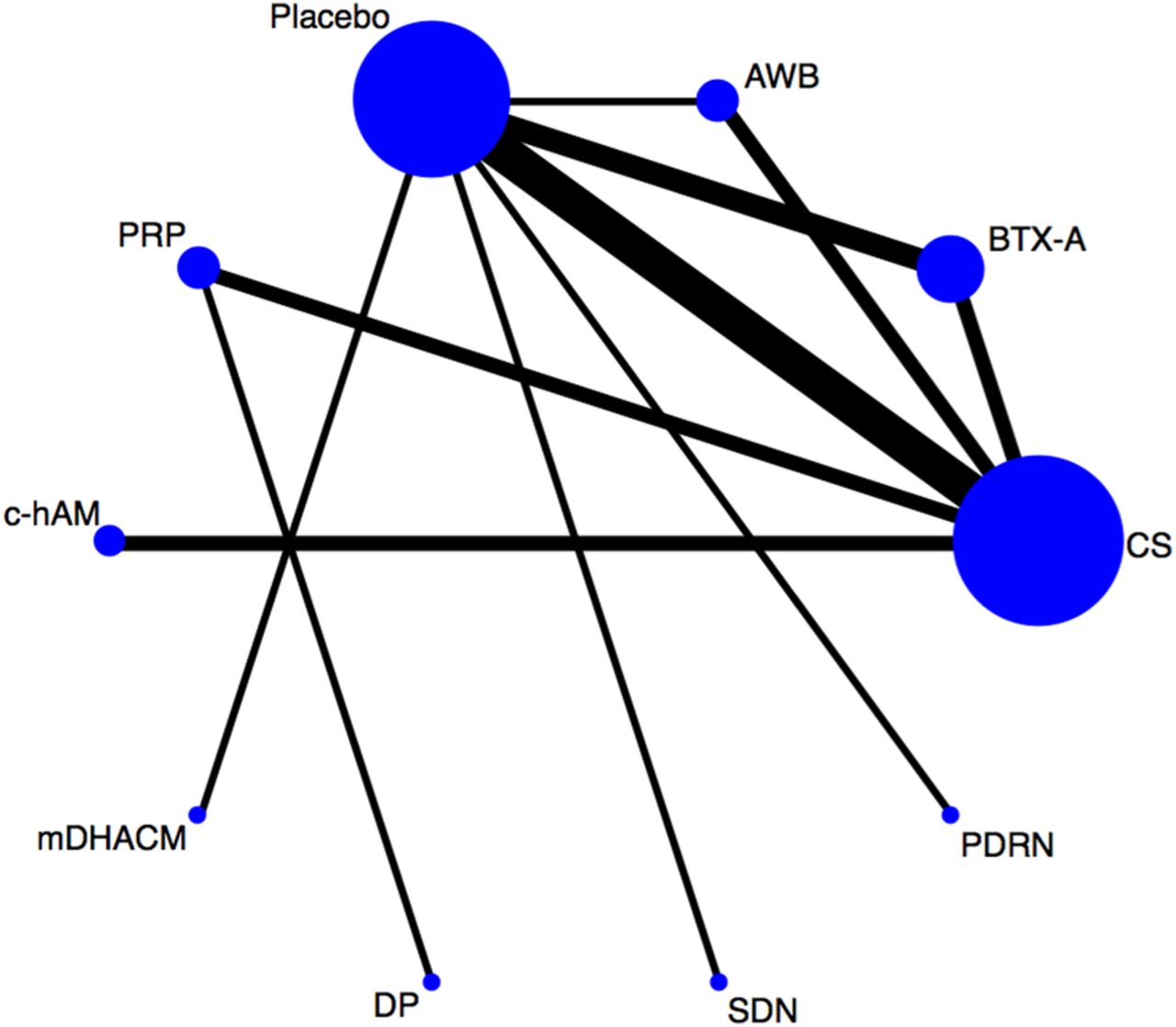
For pain relief, data for 18 RCTs comprising 1009 participants were available in the short-term assessment. We compared the relative efficacy of the following interventions in the pooled analysis: CSs, BTX-A, AWB, Placebo, PRP, c-hAM, mDHACM, DP, SDN and PDRN; figure 3). For this outcome, we detected two triangle loops in the network of interventions. The inconsistency in these loops was not statistically significant (see online supplementary file 4a).

Network meta-analysis plot for the assessment of pain relief in the short term (0–2 months). CS, corticosteroid; PRP, platelet-rich plasma; mDHACM, micronised dehydrated human amniotic/chorionic membrane; DP, dextrose prolotherapy; BTX-A, botulinum toxin-A; PDRN, polydeoxyribonucleotide; c-hAM, cryopreserved human amniotic membrane; AWB, autologous whole blood; SDN, sham dry needling.
Supplementary file 4a
The largest contribution to the network estimates (ie, 15%) stemmed from studies comparing CSs to placebo (see online supplementary file 4a). For pain relief, there was a statistically significant superiority of the dehydrated amniotic membrane, PRP and BTX-A injections over CSs at 0–2 months (MD in VAS was −7.32, 95% CIs −11.2 to −3.38, large effect size; −2.38, 95% CIs −4.66 to −0.07, large effect size; and −1.68, 95% CIs −3.29 to −0.07, large effect size, respectively). Moreover, intervention with the dehydrated amniotic membrane was significantly more effective than all treatments with the exception of DP (figure 4). This intervention was also found to be the most effective modality in relieving pain intensity at 0–2 months (figure 5). The results of the pairwise meta-analyses for the short-term assessment of pain relief are presented in online supplementary file 4a.

League table showing network meta-analysis estimates of pain relief in the short term (0–2 months). PRP, platelet-rich plasma; mDHACM, micronised dehydrated human amniotic/chorionic membrane; DP, dextrose prolotherapy; BTX-A, botulinum toxin-A; PDRN, polydeoxyribonucleotide; c-hAM, cryopreserved human amniotic membrane; AWB, autologous whole blood; SDN, sham dry needling.

Ranking probability plot for the assessment of pain relief in the short term (0-2 months). PRP, platelet-rich plasma; mDHACM, micronised dehydrated human amniotic/chorionic membrane; DP, dextrose prolotherapy; BTX-A, botulinum toxin-A; PDRN, polydeoxyribonucleotide; c-hAM, cryopreserved human amniotic membrane; AWB, autologous whole blood; SDN, sham dry needling.
As for the short-term assessment of composite outcomes, we abstracted information from 10 studies comprising 452 patients. We compared the relative efficacy of the following modalities at 0–2 months: CSs, BTX-A, Placebo, PRP, c-hAM, mDHACM, DP, SDN and PDRN. We graphically presented the network of interventions in online supplementary file 4b. In this network, the dehydrated amniotic membrane had the highest probability of being among the best injection treatments (see online supplementary file 4b).
Supplementary file 4b
For functional disability, we considered four trials with 180 participants at 0–2 months. The following competing interventions were considered in the analysis: CSs, BTX-A, Placebo, PRP, c-hAM, DP and SDN. Two head-to-head comparisons were connected to a network of interventions (see online supplementary file 4c). In this network, the BTX-A intervention was the best treatment (see online supplementary file 4c). As for the direct comparisons that were not connected to the latter network, we detected no statistically significant differences between the intervention groups (see online supplementary file 4c).
Supplementary file 4c
For health-related outcomes, we considered four trials with 202 participants. For this study outcome, two disconnected networks of interventions were created (see online supplementary file 4d). There was a statistically significant superiority of the micronised dehydrated amniotic membrane over placebo intervention at 0–2 months (MD in the FHSQ general health subscale was 49.9, 95% CIs 27.1 to 72.4, large effect size).
Supplementary file 4d
Intermediate-term outcome assessment (2–6 months)
For pain relief, we included 15 studies with a total of 800 participants in the quantitative synthesis at 2–6 months. We considered the following intervention groups in the analysis: CSs, BTX-A, AB, Placebo, PRP, NSAIDs, c-hAM, DP, SDN and PDRN (see online supplementary file 5a). There was no significant inconsistency in the two triangle loops that were detected in the network of interventions (see online supplementary file 5a). For pain relief, BTX-A was the highest ranked modality in the intermediate term (see online supplementary file 5a). For pairwise comparisons, the results of the intermediate-term assessment of pain relief are shown in online supplementary file 5a.
Supplementary file 5a
Data for 7 RCTs with 277 patients were available for the assessment of composite outcomes in the intermediate term. We considered the competing intervention groups of CSs, BTX-A, AB, Placebo, PRP, c-hAM, DP, SDN and PDRN. For this study outcome, we detected a closed loop in the network of treatments that was consistent by definition (it was formed by multiarm trials). We demonstrated that PRP was the highest ranked treatment at 2–6 months (see online supplementary file 5b).
Supplementary file 5b
Regarding the intermediate-term assessment of functional disability, we included three studies comprising 122 patients in the analysis. There were no statistically significant differences between the included intervention groups (see online supplementary 5c).
Supplementary file 5c
For health-related outcomes, we considered two RCTs with 102 patients in the intermediate-term assessment. It is noted that the intervention groups were not connected to a network of treatments. For this study outcome, we detected no statistically significant differences between the included head-to-head comparisons at 2–6 months. The results of the analyses are presented in online supplementary file 5d.
Supplementary file 5d
Medium-term outcome assessment (more than 6 months to 2 years)
In this systematic review, only two trials included follow-up observations at 28 weeks and beyond (see online supplementary file 2a).49 ,58 For pain relief, we considered two studies with 82 participants in the medium-term assessment. There was no statistically significant difference between NSAIDs and CS injections at 12 months after treatment (mean difference in VAS was −0.67, 95% CIs −1.87 to 0.55) (see online supplementary file 6a). PRP was not significantly more effective in relieving pain intensity than DP at 28 weeks after treatment (mean difference in VAS was −1.32, 95% CIs −3.48 to 0.84) (see online supplementary file 6a).
Supplementary file 6a
For the medium-term assessment of composite outcomes, we included three trials with 122 patients. For this study outcome, we created a star-shaped network of treatments (see online supplementary file 6b). PRP had the highest probability of being the best treatment in the medium term (see online supplementary file 6b).
Supplementary file 6b
For functional disability, we included only 1 trial with 20 patients in the medium-term follow-up. There were no statistically significant differences between the intervention groups (see online supplementary file 6c). It is noted that there was no available information about health-related outcomes in the medium term.
Supplementary file 6c
The results of the analyses demonstrated that there was no significant inconsistency in the networks of this study. Furthermore, we detected no asymmetry in the comparison-adjusted funnel plots of this systematic review (figure 6, see online supplementary files 4b and 5a).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison adjusted funnel plot for the assessment of pain relief in the short term (0–2 months). CS, corticosteroid; PRP, platelet-rich plasma; mDHACM, micronised dehydrated human amniotic/chorionic membrane; DP, dextrose prolotherapy; BTX-A, botulinum toxin-A; PDRN, polydeoxyri-bonucleotide; c-hAM, cryopreserved human amniotic membrane; AWB, autologous whole blood; SDN, sham dry needling.
Side effects
Overall, no major adverse effects related to the injection therapies were reported in any of the included RCTs. Of the 22 studies, 16 specifically reported the absence of serious side events related to the included treatments and 6 did not make any mention of this factor.49 ,51 ,57 ,63 ,66 ,67
The most common minor adverse effect that was reported in the included trials was that of temporary post injection pain.47 ,50 ,55 ,59 The participants in three enrolled RCTs found the injection to be painful.48 ,59 ,60
One patient was hospitalised for 2 days after receiving 0.5 cm3 of the dehydrated amniotic membrane because of severe pain behind the eye and headache.52 It was believed that this side effect was unrelated to the administration of the treatment. Between the first and seventh days after treatment, eight participants treated with dry needling and one treated with SDN experienced minor side effects (including bruising and aggravation of symptoms).50 Exacerbation of symptoms was also reported in two participants who received saline injections and in one patient treated with BTX-A injection.55
Additional analyses
The results of meta-regression analyses indicated that the regression coefficients were associated with much uncertainty. Similarly, we detected much uncertainty in the results of subgroup analyses. Thus, we performed post hoc sensitivity analyses to investigate the impact of the effect modifiers that were not fully explored with the preplanned subgroup and meta-regression analyses. The results of both the prespecified and a posteriori defined sensitivity analyses showed that inconsistency was low in all cases.
When we excluded PRP trials at an unclear risk from the analyses, the comparative efficacy and treatment ranking of this modality were decreased in the included networks of interventions.
In a sensitivity analysis excluding trials at a high/unclear risk of bias according to the elements of randomisation and masking of the participants, similar results to those of our primary analyses were demonstrated. However, there were no available trials comparing the efficacy of PRP in the latter analysis.
Discussion
Summary of main results
We identified 22 RCTs comparing the effects of various injectable therapies for the management of PF. For pain relief and composite outcomes, the dehydrated amniotic membrane, PRP and BTX-A injections were significantly superior to CSs at 0–2 months. For these study outcomes, the dehydrated amniotic membrane had the highest probability of being among the best injection treatments in the short term. For health-related outcomes, there was a significant clinical advantage of the dehydrated amniotic membrane over placebo injections at 0–2 months. Intervention with BTX-A provided significantly greater pain relief compared to placebo at 0–6 months.
Quality of evidence
In the present systematic review, we restricted our eligibility criteria to studies using an RCT design. The purpose of this restriction was to prevent systematic differences between baseline characteristics of patients in different comparison groups in terms of the confounding factors.69
In this study, we considered that the assessment of blinding of patients was critical because the outcomes that were evaluated were highly subjective in nature.13 We highlight that a significant proportion of the enrolled participants were successfully masked to the intervention they were randomly assigned to (ie, 936/1212). Consequently, the magnitude of bias associated with this domain was supposed to be decreased.13
After synthesising qualitative evidence, we proceeded to our prespecified primary meta-analyses (ie, pairwise and network quantitative syntheses). Then we incorporated bias assessment in the results of our study by performing a stratified analysis. The findings on the efficacy of BTX-A and dehydrated amniotic membrane interventions were robust enough after controlling for the quality of the included trials.
Industrial funding
Currently, there is much controversy regarding the inclusion of the funding source in the risk of bias domains.70 ,71 The Cochrane Collaboration has initiated a discussion about the possibility of including funding source as an item in the risk of bias tool. There are arguments both in favour of and against its inclusion and the Cochrane Collaboration has not made a decision. For this reason, we did not include funding source in the risk of bias assessment of our study.
Validity of the results
In this study, the results of the analyses demonstrated that there was no significant inconsistency in all cases. It is important that there is no significant inconsistency in a network meta-analysis. If significant inconsistency is present, the validity of the results may be influenced.24
Dehydrated human amniotic membrane intervention
For pain relief and composite outcomes, intervention with the dehydrated amniotic membrane was the highest ranked treatment at 0–2 months. This intervention was included in only one RCT, conducted in the USA. In this trial, there were two arms containing intervention with the dehydrated amniotic membrane at a different dosage. We combined the latter intervention groups into a single one because there was no significant difference in treatment response between these two arms.30 ,52
Dry needling intervention
Dry needling (also known as peppering) is not a widely used stand-alone therapy for PF. Although the efficacy of this intervention for the management of PF is not yet fully investigated, promising results have been published.50 ,72
We hypothesised that the needling of the plantar fascia (with or without injecting any substances) exerts a beneficial impact on the rehabilitation of PF, similar to that demonstrated on tendinopathy.73 For this reason, we included both dry needling and saline injections in the placebo arm of our study. On the other hand, we included a separate intervention arm for SDN (ie, non-penetrating sham acupuncture) because of the absence of the needling of the plantar fascia.
We tested our hypothesis by performing a sensitivity analysis in which we included only a dry needling intervention in the placebo arm of this network meta-analysis. In the latter analysis, there were similar results to those of our primary analysis. For pain relief, pooled results showed that the dry needling intervention was significantly superior to SDN at 0–2 months (mean difference in VAS was −1.99; 95% CIs −3.34 to −0.62; large effect size). These data supported our hypothesis, although conclusions were limited by the quality of two included trials on dry needling.57 ,60
Image guidance of the injections
The current literature suggests that US-guided CS injections are more effective than palpation-guided ones for the management of PF. There is strong evidence that the accuracy of US guidance is greater than that of palpation guidance.74 For these reasons, we explored the impact of this potential source of clinical diversity on the results of the present systematic review and network meta-analysis by performing a sensitivity analysis. In this analysis, we excluded head-to-head comparisons investigating the efficacy of US-guided CS injections. We detected no significant inconsistency, and we also observed no significant changes in the comparative estimates and treatment rankings.
Clinical implications
In this review, the dehydrated amniotic membrane intervention seemed to be helpful at 0–2 months. However, the paucity of information regarding the long-term efficacy and safety of this therapy did not allow us to draw safe conclusions about this modality. It is noted that the product is available for clinical use in the USA only.
If the clinician is choosing among injection options alone, BTX-A was the one most likely to relieve pain intensity compared to placebo in the 0–6-month window. There were no major unintended effects related to the administration of toxin injections during this time period.
As for PRP injections, the quality of the existing RCTs did not allow us to create safe conclusions about the efficacy of this therapy.
Physical therapy for the treatment of PF
It is strongly suggested that physical therapy is used for the management of PF. It may include stretching exercises, manual therapy, taping, foot orthoses and night splints.36 In our study, we excluded trials investigating the efficacy of physiotherapy because they did not meet our inclusion criteria.
Finally, we recommend that clinicians take into account the efficacy of the available therapies for PF, as well as the cost and the potential side effects of these treatments.
Implications for research
In this study, we found that there is a paucity of clinical information about the efficacy of injection therapies for PF at 6 months and beyond. Consequently, we highlight the need for high quality RCTs with long-term observations to explore the efficacy of injection therapies.
Furthermore, there was no available information about adverse events for approximately 25% of the included trials. For this reason, we underline the necessity for adequate reporting of unintended effects in future RCTs on injection therapies for PF.
It is also suggested that authors of future trials utilise one of the following validated PRO questionnaires for the clinical evaluation of PF: FHSQ; Foot Function Index; Foot and Ankle Ability Measure; and the computer-adaptive version of the Lower-Extremity Functional Scale.36
Our study highlights that the following sources of clinical heterogeneity should be carefully addressed in future studies: previous treatments, duration of symptoms before the intervention, the number of injections, cointerventions and postrehabilitation protocol. Grants funded by major national research agencies should take these factors into account.
There are methods for designing a future trial with the aim of informing the results from a network meta-analysis. In this case, we are interested not only in the sample size of the future trial, but also in its comparison(s).75 ,76
Study limitations
In the present systematic review and network meta-analysis, the inclusion of all eligible RCTs in the quantitative syntheses increases the statistical precision of results (ie, narrow CIs). On the other hand, the inclusion of low quality trials in the analyses may introduce bias because of the flaws in the conduct of these RCTs.13
In addition, the limited number of trials in combination with the large number of treatments did not allow us to get powerful results. As for the treatment rankings, we detected much uncertainty associated with many interventions in the rankograms (ie, flat distribution of probabilities assuming a rank).
We also avoided selecting composite outcomes, in terms of a validated PRO questionnaire, as our primary outcome measure. This was because composite outcomes were not assessed in all cases (see online supplementary file 2a).
The information from the medium-term follow-up (ie, more than 6 months to 2 years) was limited and clinically diverse. Thus, we were not able to create safe conclusions about the efficacy of the available injection therapies for PF at 6 months and beyond.
Pooled results showed that intervention with the dehydrated amniotic membrane had the highest probability of being among the most effective modalities at 0–2 months. However, this therapy was included in only one trial, in which it was compared to placebo in the short term (ie, 8 weeks after treatment). Consequently, information about the efficacy of this modality depended extensively on indirect evidence.
The findings on the efficacy of PRP should be interpreted with caution because 50% of the available information stemmed from trials at an unclear risk of bias (see online supplementary file 3). The treatment rankings and comparative estimates of this modality were decreased when we accounted for the quality of the included head-to-head comparisons on PRP. The limited reporting of side effects in trials on PRP did not allow us to draw safe conclusions about the safety of this treatment.
Summary and conclusions
In summary, the dehydrated amniotic membrane was the injection therapy with the highest probability of being superior to placebo injection over 8 weeks. Randomised trials comparing dehydrated amniotic membranes at a longer follow-up are needed to get more precise estimates about the relative efficacy of this intervention. For pain relief, intervention with BTX-A was superior to placebo at 0–6 months.
Importantly, ‘wait-and-see’ was not tested in the enrolled trials and Vicenzino77 found injection therapy to be worse than ‘wait-and-see’ in long-term tendon outcome studies. We also highlight that the included injection therapies of the present systematic review and network meta-analysis were not compared against an active physiotherapy arm.78
What are the findings?
For pain relief and composite outcomes, the micronised dehydrated human amniotic/chorionic membrane had the highest probability of being among the best injection treatments in the short term. However, there was a lack of information about the efficacy and safety of this treatment at 2 months and beyond.
Botulinum toxin-A injections provided significant pain relief to patients who suffered from plantar fasciopathy at the 6-month follow-up. This result remained robust after controlling for the risk of bias of the included trials.
Pooled results showed that platelet-rich plasma injections were effective for the treatment of plantar fasciopathy at 0–6 months. However, conclusions about this therapy were limited by the quality of the included head-to-head comparisons on platelet-rich plasma.
How might it impact on clinical practice in the future?
If the clinician is choosing among injection options alone, botulinum toxin-A was the most likely to relieve pain intensity compared to placebo in the 0–6-month window.
At present, the findings on the efficacy of the dehydrated amniotic membrane at 0–2 months are promising. More trials are needed to investigate the long-term efficacy and safety of this therapy.
References
Footnotes
Contributors KT and HSV contributed to the study selection, data extraction and interpretation of the results. KT drafted the final version of the paper that was revised and approved by all authors. All authors of this systematic review and network meta-analysis contributed to the planning and reporting of the work.
Funding DM received research funding from the European Research Council (IMMA 260559).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.