Article Text

Abstract
Objective To promote sports participation in young people, the International Olympic Committee (IOC) introduced the Youth Olympic Games (YOG) in 2007. In 2009, the IOC Consensus Statement was published, which highlighted the value of periodic health evaluation in elite athletes. The objective of this study was to assess the efficacy of a comprehensive protocol for illness and injury detection, tailored for adolescent athletes participating in Summer or Winter YOG.
Methods Between 2010 and 2014, a total of 247 unique adolescent elite Italian athletes (53% females), mean age 16±1,0 years, competing in 22 summer or 15 winter sport disciplines, were evaluated through a tailored pre-participation health evaluation protocol, at the Sports Medicine and Science Institute of the Italian Olympic Committee.
Results In 30 of the 247 athletes (12%), the pre-participation evaluation led to the final diagnosis of pathological conditions warranting treatment and/or surveillance, including cardiovascular in 11 (4.5%), pulmonary in 11 (4.5%), endocrine in five (2.0%), infectious, neurological and psychiatric disorders in one each (0.4%). Based on National and International Guidelines and Recommendations, none of the athletes was considered at high risk for acute events and all were judged eligible to compete at the YOG. Athletes with abnormal conditions were required to undergo a periodic follow-up.
Conclusions The Youth Pre-Participation Health Evaluation proved to be effective in identifying a wide range of disorders, allowing prompt treatment, appropriate surveillance and avoidance of potential long-term consequences, in a significant proportion (12%) of adolescent Italian Olympic athletes.
- adolescent
- olympics
- health promotion
- elite performance
- prevention
Statistics from Altmetric.com
Introduction
In Western countries, participation in regular exercise programmes and sport events characteristically shows a progressive reduction with ageing, starting with adolescence.1 The decrease in sport participation is associated with an increased incidence of obesity and sedentary behaviours in adulthood. Furthermore, it is known that a large proportion of teenagers do not meet the recommended physical activity minimum standard.2
To counteract this alarming trend and to promote sports participation in young people, in 2007 the International Olympic Committee (IOC) approved the creation of a youth version of the Olympic Games, for athletes between 14 and 18 years' old. So far, four editions of the Youth Olympic Games (YOG) have taken place (two Summer and two Winter Games), with growing participation and level of achievement.
In 2009 the IOC published a Consensus Statement on the Periodic Health Evaluation of Olympic athletes, clarifying the objectives and procedures of the Pre-Participation Evaluation in adults.3 The main targets of the pre-participation programme in such a context are: to timely identify silent pathological conditions, allowing for prompt intervention and management, thus minimising adverse health consequences; to exclude injuries or medical conditions that may impair the athlete’s safe participation; and finally to confirm that the athlete is medically eligible to compete to the Games.
Up to now, no similar recommendations have been published for adolescent elite athletes and very few data are available in the literature on periodic health evaluation in this population.4 Therefore, doubts exist whether the same protocol for adults should be applied to younger athletes. It is our opinion that elite adolescent athletes can be subject to substantial training loads, and they should be evaluated with as comprehensive an approach as that given to elite adult Olympic athletes.
The objective of our study was, therefore, to assess the efficacy of a tailored Youth Pre-Participation Health Evaluation (YPPHE) protocol to prevent illness and injury in Italian adolescent athletes, selected to participate in the Summer or Winter YOG.
Methods
The YPPHE programme described in this study was developed using the adult Olympic medical programme as a model. The adult version has been previously implemented at the Sport Medicine and Science Institute of the Italian Olympic Committee, CONI (Rome, Italy), for athletes selected to compete in either Summer or Winter Olympic Games, whose results have been previously reported.5–7
Study population
Italian adolescent athletes were evaluated before the Singapore 2010 Summer YOG, Innsbruck 2012 Winter YOG or Nanjing 2014 Summer YOG. A total of 259 adolescent athletes entered the YPPHE – of these, 12 were eventually excluded due to insufficient or incomplete data. The final study population therefore included 247 unique adolescent athletes.
Athletes aged 14 to 18 years (mean 16±1.0 years), competed in 22 summer or 15 winter sport disciplines, with females comprising the majority (53%). The highest participation rates in the Summer Games were seen in athletics (track and field), and in the Winter Games in downhill skiing. We divided the athletes into four groups based on sports categorisation: skill (including equestrian, shooting, sailing, curling, golf; n=43); power (weightlifting, sprinting, downhill skiing; n=62); mixed (tennis, basketball, martial arts, ice hockey; n=51); and endurance disciplines (rowing, long-distance running, cycling, triathlon, pentathlon, cross-country skiing; n=91), as previously described.5
Previous to the YPPHE, athletes had been involved in regular training and competitive events for 3 to 7 years (average, 5 years) and were training intensely at the time of our evaluation. The usual schedule included six to 10 sessions a week, for about 1 to 2 hours per session.
Written informed consent was obtained from the accompanying parent for each athlete undergoing the evaluation, compliant with Italian law and the Institute’s policies. The study design was approved by the Review Board of the Institute and funded by the Italian National Olympic Committee. All clinical data assembled from athletes are maintained in an institutional database.
The Youth Pre-Participation Health Evaluation
Each athlete was evaluated on a full single day, at the Sports Medicine and Science Institute of the Italian Olympic Committee, CONI, in Rome, Italy. Evaluations and tests were performed by specialists with extensive experience in working with elite athletes. A team of medical specialists and sports psychologists was available on site or on a consultation basis.
Sports medicine evaluation
General physical examination with personal and family history was performed by a sports medicine specialist, according to the recommendations of the IOC.3 Blood pressure was measured according to the ESH/ESC guidelines.8
Anthropometric and nutritional evaluation
Physical examination included body mass index and body composition measurement through air displacement plethysmography performed with a Cosmed BOD-POD (Cosmed, Rome, Italy). Body fat and lean percentages (%) and absolute values (kg) were measured, as recommended.9 The anthropometric and nutritional examination included investigation of dietary habits, estimated daily energy expenditure and energy intake through previously described methodology.10
Cardiovascular evaluation
The cardiovascular examination was performed by an experienced cardiologist and comprised a physical examination and a 12-lead ECG, performed with the subject supine during quiet respiration, at 25 mm/s, using a Cardioline ClickECG, (Cardioline, Italy). ECG analysis was performed adopting international criteria11–14 to identify abnormal ECG patterns in athletes.
The exercise testing was carried out through an incremental protocol until exhaustion performed on a bicycle ergometer (Cardioline XR400, Cardioline, Italy). ECG was recorded continuously during exercise and the following 7 min of recovery.
Echocardiography was performed using iE33 (Philips Medical System, Andover, MA). The assessment included two-dimensional measurements of cardiac structures, left ventricle (LV) mass and ejection fraction. These were performed as recommended by the American Society of Echocardiography/European Association of Cardiovascular Imaging guidelines.15 Tissue doppler imaging signals and LV inflow velocities were registered in the apical four-chamber, as described in the literature.16
Pulmonary and allergy evaluation
Pulmonary and allergy examination included personal, family history and physical examination with special reference to the presence of sensitisation and allergic diseases, asthma, upper respiratory tract infections and autoimmune diseases. Clinical, functional and immunological parameters were collected, using pulmonary function test and skin test reactivity to common allergens, as for adult athletes.17 Spirometry was performed with a Quark PFT2 spirometer (Cosmed, Rome, Italy) according to the standardised criteria proposed by the American/European Respiratory Society.18 Forced vtal capacity (FVC), peak expiratory flow, forced expiratory in 1 s (FEV1), FEV1/FVC and maximal mid-expiratory flow (MMEF25-75) were recorded from the best of the first three technically sufficient flow-volume loops.
Bronchial challenges were performed in all those subjects with a suspected diagnosis of asthma or exercise-induced bronchoconstriction. The bronchodilator test was performed by measuring FEV1 15 min after 200 mcg inhaled salbutamol. The methacoline test19 and the indirect bronchial provocation tests (exercise challenge, eucapnic voluntary hyperventilation and mannitol)20 were selectively performed only in subjects with FEV1 <80% of predicted.
Skin prick tests were performed according to the standard procedure and panel of allergens defined by the GA2LEN European Network of Excellence.21
Orthopaedic evaluation
Orthopaedic examination was performed by an orthopaedic surgeon. It was tailored to the sport practised and based on the individual characteristics of the subject evaluated. It included history of previous injuries, concussion episodes or pubertal growth conditions and a thorough musculoskeletal physical examination.22 Specifically, physical examination aimed at evaluating flexibility and muscle strength, growth asymmetries, abnormal posture or foot configuration.23–25
Ophthalmological evaluation
Ophthalmological examination included the assessment of visual acuity, visual fields, previous occurrence of infective and allergic eye diseases, and funduscopy.
Ear, nose and throat evaluation
The ear, nose and throat examination aimed at detecting the occurrence of infectious or allergic diseases. The physical examination included assessment of the external auditory canal, tympanic membrane, sinuses, nasal septum, turbinate bones, oropharynx, tonsils, cervical and regional lymphadenopathy, as well as indirect laryngoscopy (if deemed necessary).
Psychological evaluation
The psychological examination was performed through the Self-Esteem Multidimensional Test (TMA) which was administered by a sports psychologist during a colloquium.26 The TMA is based on a hierarchical model of self-esteem. It comprises six self-esteem dimensions (Personal, Skills, Emotional, School, Family, Body, Total) that partly overlap each other and partly with the core global self-esteem. The test provides scores in six rating scales corresponding to the cited six self-esteem dimensions and a global self-esteem-related score.
Urine and blood tests
Each athlete collected a first morning urine specimen on the same morning of the evaluation. These specimens were analysed in duplicate for osmolality, specific gravity and colour.
A blood sample was also collected from each athlete the same morning of the evaluation, following a minimum 12 hours' fast. Complete blood count, ferritin levels, glycaemia, coagulation, inflammatory, liver, renal, lipid, thyroid and electrolyte profiles were performed.
Finally, in selected athletes, further specialist evaluations were performed, such as endocrine/gynaecological evaluation in female athletes, dermatological evaluation in athletes practising outdoor sports or at prolonged sunlight exposure, and dental and neurological evaluation in athletes engaged in contact disciplines (such as martial arts).
Once these other specialists’ evaluations were completed, the sport medicine specialist reviewed the results of the investigations and, in the absence of major contraindications, confirmed the eligibility of the athlete to compete at the coming YOG.
Statistical analysis
The study design was a retrospective analysis of the prevalence of relevant abnormalities and/or diseases found among adolescent Italian Olympic athletes. Continuous data are expressed as mean ±SD. Gender differences were evaluated by unpaired-samples t-test. Differences between sport disciplines were evaluated using Analysis of Variance. Differences between proportions were evaluated by the Chi-square test. Statistical analysis was performed using SPSS (version 22, SPSS Inc. Chicago IL, USA) and statistical significance was set at P<0.05.
Results
Demographic and anthropometric characteristics
Athletes’ age was 16±0.9 (14–18) years in males and 16±1.0 (13–18) in females. Mean measures of weight, height and body surface area for males were greater than for females. Body fat percentages were within the optimal range for both groups, based on gender, age and ethnicity criteria.27 28 Systolic and diastolic blood pressures were relatively higher in males, while heart rate was similar in both groups (table 1).
Demographic and anthropometric characteristics of 247 adolescent Olympic athletes according to gender
When analysed by type of sport, athletes competing in mixed disciplines showed the largest body size. Percentage of body fat was significantly lower in endurance athletes compared with other sport disciplines. Endurance athletes also showed a significantly lower heart rate and relatively higher blood pressure (table 2).
Demographic and anthropometric characteristics of 247 adolescent Olympic athletes according to type of sport participated
Clinical findings
The majority of the 247 athletes, (n=171, 69%) had completely normal findings. A relevant group of athletes, (n=46, 19%), showed a wide spectrum of minor abnormal findings that were nevertheless investigated and considered, in the end, not clinically relevant. The remaining 30 athletes (12%) presented abnormalities that led, after completion of the diagnostic process, to identification of a disease condition. These were cardiovascular in 11 (4.5%), pulmonary in 11 (4.5%), endocrine in 5 (2.0%), and infectious, neurological and psychiatric disorders in one each (0.4% each) (figure 1).

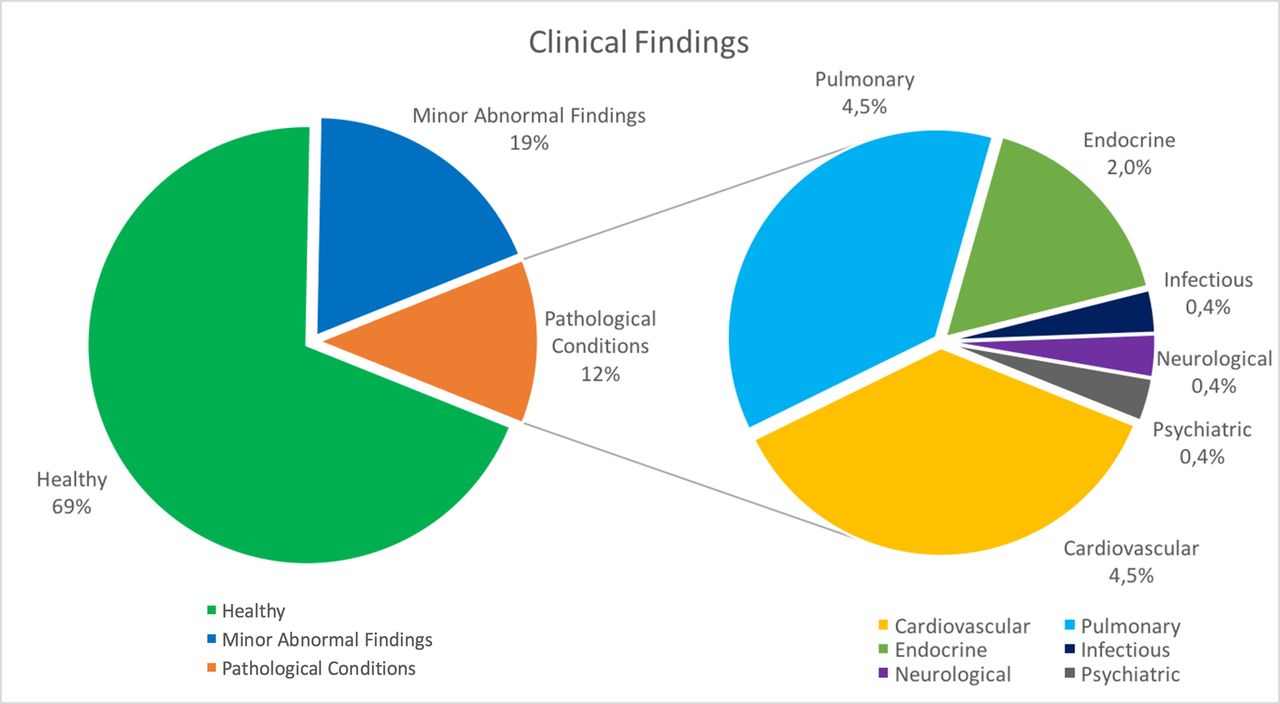{kind=link}
The results of the Youth Pre-Participation Health Evaluation in adolescent Olympic athletes. Permissions Information: ’The authors do hereby declare that all illustrations and figures in the manuscript are entirely original and do not require reprint permission.’
Cardiovascular findings
Cardiovascular abnormalities were found in 11 (4.5%) including mitral valve prolapse without relevant regurgitation in three (1.2%), bicuspid aortic valve (BAV) with mild regurgitation in three (1.2%) and atrial septal defect with left-to-right shunt in 1 (0.4%). Among athletes with a BAV, one had associated a mild stenosis (peak gradient, 25 mmHg), but normal ascending and thoracic aorta dimensions. All these athletes were required to undergo a periodic follow-up.
Three subjects (1.2%) presented with a primary electrical disorder: specifically, one with ventricular pre-excitation; one with non-sustained ventricular tachycardia (NSVT); and one with supraventricular reciprocating tachycardia (SVT). The athlete with ventricular pre-excitation underwent an electrophysiological study and was judged to be at low risk. The athlete with NSVT had also infero-lateral T-wave inversion at 12-lead ECG, which prompted examination with cardiac magnetic resonance, which excluded structural/functional cardiac abnormalities. The athlete was advised to have periodic follow-up evaluation. The athlete with SVT complained of palpitation and chest discomfort during training. A diagnostic electrophysiological study confirmed the presence of a slow nodal pathway causing an atrioventricular nodal re-entry tachycardia that was successfully treated with cryoablation. At re-evaluation after 6 months the athlete was asymptomatic and showed no significant arrhythmias.
Finally, systemic hypertension was diagnosed in one overweight athlete with blood pressure (BP) values consistently ≥140 and ≥90 mmHg on repeated measurements.8 The ambulatory 24-hour BP monitoring confirmed the high systolic and diastolic BP values during both day and night (24 hours' mean value, 144/92 mmHg). Weight loss, low sodium diet and periodical monitoring of the BP values were prescribed.
Pulmonary-allergy findings
Allergic asthma was initially suspected in 11 athletes (4.5%) and the diagnosis was confirmed based on bronchial challenges and according to the criteria of the Global Initiative for Asthma (GINA) guidelines.29 Athletes with exercise-induced bronchoconstriction were considered asthmatic patients, even in the absence of asthma at the time of evaluation. Rhinitis, conjunctivitis, allergic skin diseases, anaphylaxis and autoimmune diseases were diagnosed according to international guidelines, with special reference to the criteria set for athletes.30 31 Athletes were defined as allergic in the presence of at least one positive sensitisation to allergens at skin tests. Allergic athletes were prescribed long acting ß2-agonists, inhaled corticosteroids, leukotriene receptor antagonists or antihistamines, based on individual characteristics and symptoms.
Endocrine-metabolic findings
Five athletes presented with a variety of endocrine conditions, including Hashimoto’s thyroiditis in two, hypothyroidism in two and Complete Androgen Insensitivity Syndrome (CAIS) in one. Hashimoto’s thyroiditis and hypothyroidism diagnoses were based on the abnormal thyroid hormonal levels found in blood tests. All athletes were asymptomatic and based on the residual thyroid functionality were prescribed levothyroxine. The athlete with CAIS was diagnosed at birth and was under treatment with ethinylestradiol.
Other medical conditions
One athlete (0.4%) had materno-fetal transmission of hepatitis B. All liver functionality parameters were normal as well as abdominal ultrasonography. Hepatitis B Ag markers (HBsAg) were the only positive markers found in the blood test. The athlete was not in treatment.
Neurologic findings
One athlete (0.4%) was affected by epilepsy that was diagnosed following two episodes of generalised seizure that were both prompted by sleep deprivation periods. The athlete was treated with controlled release valproic acid with complete resolution of the clinical picture and absence of recurrences. The neurologic physical examination was normal as well as the electroencephalogram.
Psychiatric findings
One athlete (0.4%) showed very low results on psychological tests, with critical values in all areas of the self-esteem TMA test. An initial depression syndrome characterised by several panic attacks was diagnosed. Furthermore, the athlete reported feeling overwhelmed and stressed by the responsibility and expectations of the surrounding environment. The athlete was under treatment with sertraline, oxazepam and lormetazepam and periodic assessment by a specialist psychiatrist.
Sport participation
Sport participation and follow-up management of athletes was advised based on current national and international recommendations.32–40 None of the athletes was considered to be at risk for acute events and all were judged eligible to compete at the YOG.
Athletes with pathological conditions or abnormal findings were required to undergo a periodic follow-up at either 6 or 12 months, based on the diagnosed condition, individual characteristics and according to the aforementioned recommendations.
Discussion
In the present study we report the first experience of a tailored medical protocol for adolescent Olympic athletes, to assess their health condition and potentially prevent sport- related injuries and illnesses, in accord with the dictates of the IOC.3 Our youth medical protocol was developed and implemented based on the adult Olympic protocol5 and following the IOC suggestions, taking into account the physiological and psychological characteristics of young athletes through an adapted approach that considers the ‘…constantly changing base of normal physical growth, biological maturation and behavioural development…'.41 The battery of evaluations and tests included in the protocol is a direct result of the experience in the pre-participation evaluation of Olympic athletes gathered since the late 1960s at the Sports Medicine and Science Institute in Rome.5 6
The implementation of the YPPHE programme was a decision of the Italian National Olympic Committee, in order to detect and manage any health issue that might compromise the athlete’s physical performance, with the objective of maximising the athlete’s chances of success at the YOG. Actually, the implementation of the programme was not the result of a cost-effective analysis, but a proactive initiative of the Olympic Committee, aimed to prevent illness and promote healthy behaviours in the young athlete population. This approach is consistent with the Italian healthcare and welfare systems, where the programme of athletes' pre-participation evaluation and medical care has been implemented since 1983.42 The programme is entirely funded by the Italian Olympic Committee and it might be considered an investment in the health and performance of Italian elite athletes.
The main result of the present study is the rather high prevalence (12%) of a wide range of clinical abnormalities found in a population of asymptomatic, apparently healthy, adolescents selected for participation to the YOG. Although none of the diagnosed conditions were considered to be life-threatening, our medical programme allowed for the prompt detection and early treatment of a wide range of clinical abnormalities, thus minimising potential long-term adverse consequences. Furthermore, several conditions that warrant annual surveillance were identified.
In addition to the objectives stated by the IOC3 regarding periodic health evaluation, our pre-participation health evaluation had the further objective of reassuring athletes, families, coaches and teams of the condition of the athletes' overall health and capability for safe sports participation.
We are aware that ineligibility to compete is an extreme, although sometime necessary, measure that, especially at this young age, can have devastating psychological consequences. Bearing this in mind, we were ready to implement all possible therapeutic and monitoring solutions that could reasonably allow athletes to continue participating and competing in their sport safely. This positive and constructive approach, where athletes, families, coaches and teams are aware and involved in the discussion and management of the results of the pre-participation health evaluation, is encouraged.
Furthermore, our study demonstrates that the pre-participation health evaluation needs to be tailored to the athlete population, considering age, sex, physical characteristics, physiological growth and psychological burden that athletes might be subject to, as it is in other populations.6 43 Adolescence itself can be a stressful time of life and competitive sport, through time-consuming practices, excessive travel and overloaded schedules, can further increase that stress. Frequently all these factors have a cumulative effect, that can lead to injuries, burnout and, unfortunately too often, sport dropout.44
To counteract this alarming trend and to imprint an innovative attitude to youth sport participation, the IOC published in 2015 a consensus statement on youth athletic development.41 Interestingly and for the first time in the Olympic movement, it is stated that the goal is to: '…develop healthy, capable and resilient young athletes, while attaining widespread, inclusive, sustainable and enjoyable participation and success for all levels of individual athletic achievement’. This is an objective that seems to go beyond pure competition and results, but closer to the spirit of ‘sport for all’.
Finally, certain limitations of this study are worth mentioning, including the cross-sectional design and the lack of appropriate follow-up data, which are needed to clarify the cost/efficiency and the clinical value of the diagnostic evaluations performed in this selected group of young elite athletes. Therefore, further studies are required to prove the financial legitimacy of the programme here described. Moreover, the programme implemented for young athletes was made possible in the unique setting of the Institute of Sport Medicine and Science, where a similar programme has been already implemented for adult Olympic athletes, thus minimising the costs and logistics requirements. It is doubtful that a similar programme may be easily implemented in a different scenario, particularly in developing countries.
Some limitations might apply also to the selection of tests performed on athletes, in particular in those areas of medicine where a cut-off between normal and abnormal is not clearly dichotomous.45 In these cases, the examining physician’s experience and skill are key and should adhere to good medical practice.
Moreover, it is important to remember that the relatively high prevalence of certain pathologic conditions may be related to the Italian population, a homogenous Caucasian cohort and that our results may not likely be predictive of the findings detectable in athletes of a different ethnic origin and lifestyle.
In conclusion, youth sport participation provides undeniable positive effects on fitness, health, psycho-social development, academic results, personality growth and many other aspects of life.46–50 Nevertheless, this study demonstrates that reaching the Youth Olympic competitive level does not guarantee the absence of relevant medical conditions that could adversely affect health and performance. Therefore, a tailored pre-participation health evaluation programme, such as the one described in the current study, may be considered for early identification of a wide spectrum of conditions, allowing prompt treatment or necessary surveillance to minimise negative health consequences.
What are the findings?
Adolescent athletes when competing at an elite level should be evaluated through a comprehensive pre-participation health evaluation tailored to their individual characteristics and sport practised.
Adolescent elite athletes, although capable of astonishing performances, may harbour clinical conditions that require constant follow-up and monitoring.
This study provides important new information on the prevalence of a wide range of disorders, allowing prompt treatment, appropriate surveillance and avoidance of potential long-term consequences.
How might it impact on clinical practice in the future?
Protocols for testing adults which have been adopted to evaluate adolescent athletes should take into consideration that in this population there is a constantly changing base of normal physical growth, biological maturation and behavioural development.
The preventive approach adopted in this study, strongly supports the adoption of a tailored evaluation model for adolescent Olympic athletes aimed at the detection of clinically relevant conditions and disease prevention.
Ineligibility to compete is an extreme, although sometime necessary, measure that can have devastating psychological consequences. Therefore, all possible therapeutic and monitoring solutions that could reasonably allow athletes to continue participating and competing in their sport safely, should be implemented.
References
Footnotes
Contributors All authors have contributed equally to the collection of data. Data analysis was performed by PEA, FMQ and CP. Drafting of manuscript was performed by PEA, VM and MRS. Images were designed by PEA and EL. Revision of the manuscript was performed by PEA, AP, FMDP and BDG. All authors have approved the final submission of the manuscript and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Data analysis was performed by PEA, FMQ and CP. Drafting of the manuscript was performed by PEA, VM and MRS. Images were designed by PEA and EL. Revision of the manuscript was performed by PEA, AP, FMDP and BDG. All authors have approved the final submission of the manuscript and agree to be accountable for all aspects of the work. The study design was approved by the Review Board of the Sports Medicine and Science Institute of the Italian National Olympic Committee. All clinical data assembled from athletes are maintained in an institutional database, according to Italian national privacy laws and EU GDPR. Datasets were accessible to authors onsite as they contain clinically relevant patients’ information. No additional unpublished data from the study are available. The pre-participation health evaluation programme here presented is entirely funded by the Italian National Olympic Committee in the framework of the activities aimed at promoting and safeguarding Olympic athletes’ health. Patients were not involved in the study design as this research was a retrospective analysis of the clinical findings from a pre-participation health evaluation. The lead author affirms that the manuscript is an honest, accurate and transparent account of the study being reported, that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been explained.
Patient consent Next of kin consent obtained.
Ethics approval Institute of Sports Medicine and Science Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement PEA had full access to all of the data in the study and takes responsibility, on behalf of all authors, for the integrity of the data and the accuracy of the data analysis.