Article Text

Abstract
Background Ankle injuries are prevalent in elite volleyball and suggested to result from player contact at the net. Traditionally, ankle sprains are thought to happen in a plantarflexed position, but case studies suggest plantarflexion may not be involved.
Aim Describe the injury situations and mechanisms of ankle injuries in world-class volleyball based on systematic video analysis of injuries reported through the Fédération Internationale de Volleyball (FIVB) Injury Surveillance System.
Methods Videos of 24 injuries from major FIVB tournaments were included for analysis (14 men, 10 women). Five analysts reviewed the videos to determine specific situations and mechanisms leading to injuries.
Results The majority of injuries occurred during two volleyball situations, blocking (n=15) and attacking (n=6). Injuries to blockers were the result of landing on an opponent (n=11) or teammate (n=4). Attacking injuries most frequently occurred when a back-row player landed on a front-row teammate (n=4 of 6). When landing on an opponent under the net, the attacker landed into the opponent’s court in 11 of 12 situations but without violating the centre line rule. Injuries mostly resulted from rapid inversion without any substantial plantarflexion.
Conclusions The majority of injuries occur while blocking, often landing on an opponent. The attacker is overwhelmingly to blame for injuries at the net secondary to crossing the centre line. Injuries while attacking often result from a back-row player landing on a front-row teammate. Landing-related injuries mostly result from rapid inversion with the absence of plantarflexion.
- ankle
- sprain
- risk factor
- volleyball
- injury prevention
Statistics from Altmetric.com
Introduction
Acute ankle sprains are the most prevalent injury type in volleyball,1–5 accounting for 29%–54% of all time-loss injuries among competitive players.1 3 5 In 2010, the Fédération Internationale de Volleyball (FIVB) Injury Surveillance System (ISS) was established. Modelled after International Olympic Committee (IOC) protocols,6 the ISS provides information on the rate and patterns of injuries during FIVB competitions. Data from the ISS document that ankle injuries account for 25.9% of all injuries among world-class players.4
Volleyball players are at particular risk for ankle sprains due to sport-specific tasks, such as blocking and spiking.1–3 5 7–9 Questionnaire data from the elite national level in Norway,9 Sweden2 and Denmark8 suggest that ankle sprains are often the result of player contact at the net, for example, when a blocker lands on the foot of a teammate or opposing attacker. However, no data are available on highly skilled players at the international level. Also, injuries happen quickly and often involve other players, limiting the reliability of questionnaire data from players or witnesses.10 11 To fully understand the mechanisms of ankle injuries and reduce the risk of injury to volleyball players, a more accurate description of the playing situations and mechanisms typically leading to injury is needed.
Furthermore, lateral ankle sprains are traditionally thought to result from ankle inversion in a plantarflexed position. However, case studies that have examined the specific kinematics associated with ankle sprains have contrasted this. Using model-based image-matching of injury videos12–14 and marker-based motion analysis of actual injuries during running and cutting manoeuvres,12 15 they have described the injury as occurring in a neutral or dorsiflexed position.
To best understand the factors surrounding ankle sprains, it is recommended to perform a detailed video analysis of actual injury situations.10 11 Systematic analysis of ankle injuries has been performed in football,16 but never in sports predominantly involving landing-related injuries.
Therefore, the aim of this study was to describe the injury situations and mechanisms for ankle injuries in elite volleyball based on systematic analyses of videos of injuries reported through the FIVB ISS.
Methods
Injury and video recording
We analysed video recordings of injuries to the ankle that were reported through the FIVB ISS from all major men’s and women’s senior-level tournaments (World Championships, World Cup, World Grand Prix, World League and Olympic Games) from September 2010 through November 2014. Junior-level tournaments were excluded as video recordings were not available. There were 34 major FIVB tournaments during this period and the ISS protocol was followed in 23 of these. The Men’s and Women’s World Olympic Qualification Tournaments were excluded as videos were not available. The FIVB ISS is based on prospective registration of injuries, where the medical staff of participating teams are requested to provide daily reports on all newly incurred injuries among their players.4 A newly incurred injury is defined as any musculoskeletal complaint newly sustained during match play and/or training during the event that received medical attention, regardless of the consequences with respect to absence from competition or training. Pre-existing, not fully rehabilitated injuries are not recorded.
We requested video footage from the FIVB archives of all ankle injuries with subsequent time loss (n=32); of these, 27 were available on video. Video review revealed that the injury situation was not visible in two cases and unclear in one case, resulting in 24 acute ankle injuries available for analysis. These 24 injuries included 3 injuries that were captured from one camera angle, 8 from two camera angles, 9 from three angles, 3 from four angles and 1 from six camera angles.
Video processing
The video recordings were received on DVDs as digital files of varying formats. The discs were converted using a USB 3.0 capture device and stored as AVI files. By using a video editing program (Vegas Pro 13, 64-bit; Sony Creative Software, Middleton, Wisconsin, USA) we produced two versions of each injury situation, one full version showing the entire rally from the time of serving and one short version showing the specific injury situation from all available camera angles. The video files were rendered and saved as MPEG-4 files, which allowed frame-by-frame review using QuickTime 7 (Apple, Cupertino, California, USA).
Video analysis
Five experts in the field of volleyball and sports medicine participated in the video analysis. First, three of the experts watched the videos independently and proposed a specific frame in which they believed the ankle injuries occurred. Second, these three experts reviewed the videos together and came to a consensus regarding the index frame. This was defined as the first frame in which an abnormally large movement had occurred outside of the expected normal range of physiological motion.
Third, all five analysts were asked to independently review the videos and complete an assessment form for each case. The analysts were provided basic injury information regarding the injured player’s sex, team, player number, involved ankle (left/right), position (libero/defensive specialist, middle, opposite, outside, setter) and the specific index frame and any corresponding index frames where the injury was observed.
The assessment forms included a combination of open and closed questions which evaluated the playing situation, centre line infringement and the mechanism of injury. The injury situation variables examined included playing situation (blocking—lands on opponent/teammate, back-row attack—lands on teammate, front-row attack—lands on opponent, non-contact landing, collision/contact with teammate, other), row (back/front), offence/defence, court position (1–6), ankle bracing (yes, no, unclear) and questions evaluating blocking related injury situations (blocker landing on 1 or 2 feet and the number of blockers). Injuries resulting from landing on an opponent included questions assessing whether the involved attacker and blocker landed on the centre line, landed into the opponent’s court and if there was a centre line violation.
The injury mechanism variables primarily examined lower extremity (ankle, knee, hip) joint positions at first contact with the ground or with another player’s shoe, lower extremity joint positions at the index frame and lower extremity joint movement between initial contact and the index frame. Other injury mechanism variables assessed included the timing of whether the ankle was rapidly driven into inversion or eversion after movement into a neutral flexion position, the position of the arms (overhead, shoulder level, down at side of body) and the weightbearing status of the lower extremities at the index frame (non, partial <33%, moderate=33%–67%, significant/full weightbearing >67%).
In describing the motion about the foot and ankle, we used terminology consistent with that used by Delahunt et al 17 and endorsed by the International Ankle Consortium.18 Dorsiflexion and plantarflexion were defined as the motions parallel to the sagittal plane, around a medial-lateral axis of rotation.19 Adduction and abduction of the foot occurred about a vertical axis through the shaft of the tibia with adduction resulting in an inward rotation of the foot and abduction resulting in an outward rotation of the foot.19 Inversion and eversion were defined as frontal plane motions in which inversion raises the medial border of the foot while eversion raises the lateral border of the foot.19 Supination and pronation were defined as the triplanar motions about the subtalar joint, with supination consisting of plantarflexion, adduction and inversion and pronation comprising dorsiflexion, abduction and eversion.19
After individual assessment of the cases, the results were collated. If four or five of the reviewers came to the same conclusion, agreement was said to have been reached. In the case of three reviewers having the same conclusion and no other options were chosen by more than one reviewer, agreement was deemed to also have been reached.
Finally, three of the experts met to review cases where agreement was not reached from the completed forms. Each video was viewed as many times as needed by the analysts until consensus was determined. If all three experts agreed after reviewing the video together, agreement was said to have been reached. If not, the result was deemed ‘unclear’.
Results
Ankle injury characteristics
A total of 24 injury cases were included in the video analysis, 14 men and 10 women (table 1). Injury characteristics included 11 injuries to the left ankle and 13 injuries to the right ankle. The majority of ankle injuries were to front-row players (n=20) compared with back-row players (n=4). Of the 24 injury cases, 20 resulted from one player landing on another player, 2 included non-contact landings (1 jump set, 1 back-row attack), 1 injury occurred during a small, celebratory hop after the play, and 1 was a collision between teammates in which the player diving after a tipped ball slid into his teammate’s lower leg. Most of the 24 injuries occurred during one of two volleyball situations, blocking (n=15) or attacking (n=6) (table 1).
Playing situation and injury information for 24 cases of ankle injuries in world-class volleyball
Blocking injuries
The 15 injuries to blockers were all related to the blocker landing on another player. These included 11 cases in which the blocker landed on an opponent (figure 1) and 4 cases where the blocker landed on a teammate. In 10 of these 15 cases, the blocker was injured landing primarily on one foot, whereas the blocker landed on 2 feet in four cases and was unclear in one situation. Observation of the four cases where a blocker is injured landing on a teammate revealed that the middle blocker was late to block and drifting laterally in all four incidents. In two of these situations, the middle blocker was injured; in the other two the teammate was injured. Figure 2 reveals a typical situation, where the middle blocker is injured landing on a teammate.

Injury situation: middle blocker (in red) landing on the foot of an opposing attacker who has landed on the centre line and partially into the injured player’s court. (A) Left ankle of middle blocker in plantarflexion just prior to landing. (B) Initial contact with opponent’s foot, ankle plantarflexed. (C) Left ankle in neutral ‘foot flat’ position. (D) Left ankle in inverted position following rapid inversion moment. The videos from which these figures have been taken are available online as supplementary material.

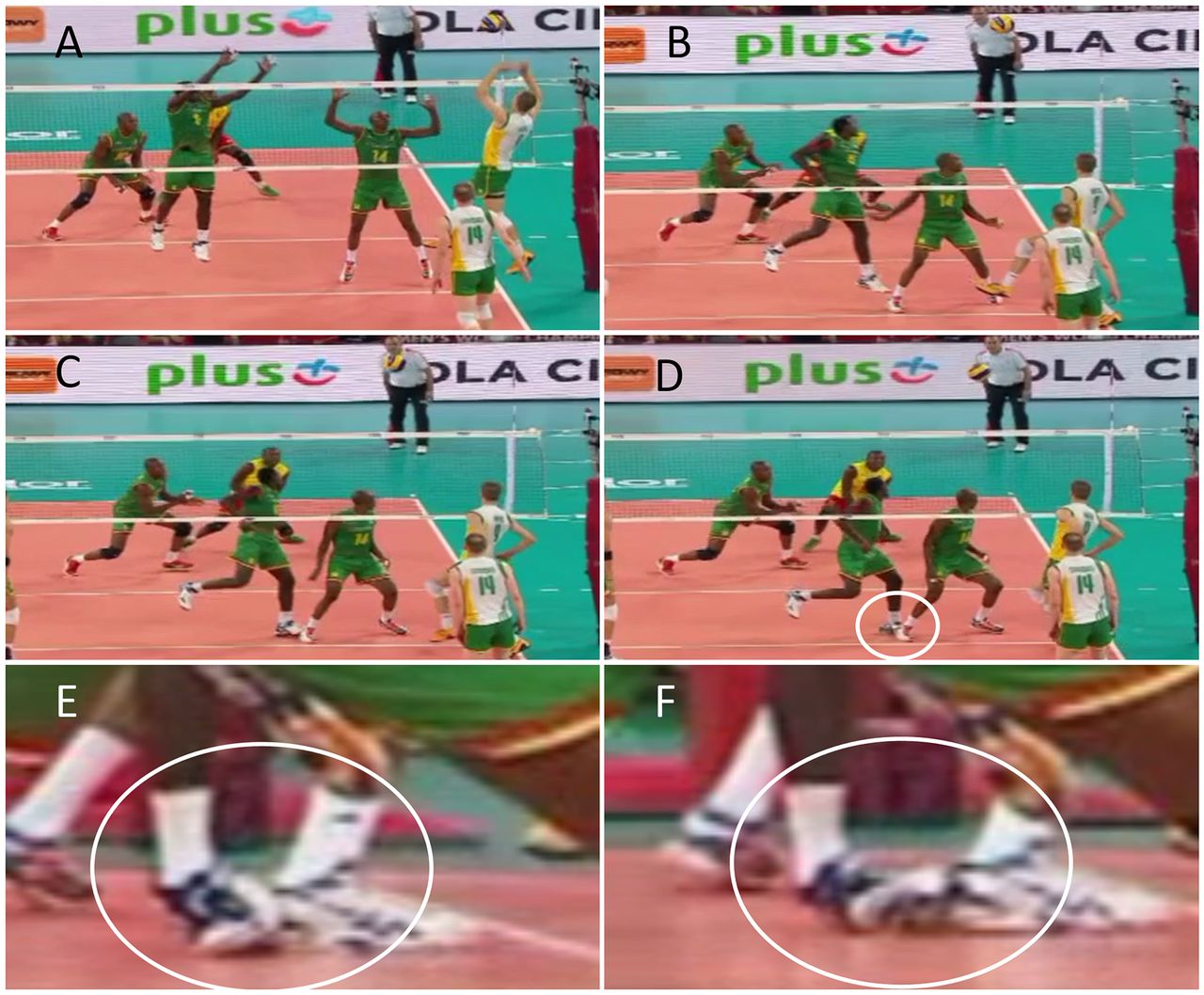
Injury situation: middle blocker landing on teammate. (A) The middle blocker jumps laterally to attempt to block the opposing player’s attack. (B) The left ankle of the middle blocker immediately prior to landing on the back of his teammate’s shoe. (C) Left foot flat on ground and ankle partially inverted. (D) Moment of injury following rapid inversion moment. (E, F) Alternate views of left ankle inversion injury taken from camera placed behind and to the right of the injured blocker’s position and correspond to images (C) and (D).
Attacking injuries
There were six cases where attacking players were injured. In five of these, the attacker was hitting out of the back row. In four of these cases, a back-row player landed on a front-row teammate; three leading to the back-row attacker being injured and one situation where the front-row player was landed on and injured. Figures 3 and 4 show two of these situations. During all four cases where a back-row attacker landed on a front-row teammate, it was observed that the offence developed out of system,20 in which the play during the rally took the team away from running the preferred pass, set, hit sequence. Of these four cases, three resulted in the player landing on the front-row middle blocker and one resulted in the setter being landed on. There was one remaining attacking injury case, which included a front-row attacker who landed on a blocking opponent at the net.

Injury situation: player landing on front-row teammate during back-row attack. (A) Overview of playing situation after attacker jumps from behind the 3 m line (white line) and just prior to ball contact. (B) The involved player contacts the ball. (C) The injured player at initial contact with front-row middle hitter, who is attempting to cover her attack. (D) Moment of injury, where the back-row player’s right ankle has inverted after landing on the right foot of her front-row teammate.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Injury situation: player landing on front-row teammate during back-row attack. (A) The involved player (red #4) begins his approach as the ball is set from the back row during a broken play. (B) Involved player begins to jump from beyond the 3 m line. (C) Involved player makes contact with ball as the front-row middle moves into the landing path while attempting to cover the hitter’s attack. (D) Moment of injury where the left foot of the injured player lands on top of the back of the left foot of his front-row teammate.
Centre line infringements
There were 12 injury situations which resulted in a player landing on an opponent under the net (table 2). The majority of these were blockers landing on opponents (n=11), with one situation of an attacking player landing on an opponent. In all 12 situations, the attacking player landed on the centre line, compared with 6 situations where the blocker landed on the centre line. Furthermore, in 11 of the 12 situations the attacker landed partially into the opponent’s court while only 2 of the situations resulted in the blocker landing partially into the opponent’s court. None of the 12 cases resulted in a centre line violation call from the officials and in none of the cases was a centre line violation by either player observed in the video analysis.
Landing position of the attacker and blocker relative to the centre line and opponent’s court
Landing-related injury mechanisms
Of the 24 injuries observed, 21 were landing-related injuries that involved the injured player landing from a traditional volleyball play which included attacking, blocking and setting. These landing-related injuries included 19 situations where the injured player landed on another player and 2 occasions where the injured player landed without any contact with another individual.
Table 3 shows the information on the mechanism for these 21 landing-related injuries in addition to the other 3 injuries observed on video. These included 18 inversion injuries and 1 eversion injury (2 injuries were unclear from the videos obtained). At initial contact by the foot with either the ground or shoe of another individual, the ankle was in a relatively neutral position in 16 situations and an inverted position in 3 situations. At initial contact the ankle was also in plantarflexion in 15 cases and in dorsiflexion in 3 cases. When examined from the point of initial contact of the foot to the index frame, the ankle moved toward dorsiflexion in 16 cases, remained in a static position in 2 cases and was unclear in 3 additional situations. Of the 19 situations where a player landed on another player, it was determined that the ankle first moved into a neutral dorsiflexed position prior to rapid inversion/eversion in 15 situations compared with 1 situation in which the ankle was not first in a neutral dorsiflexed position (3 situations were unclear).
Injury mechanisms for the involved ankle and limb during ankle injuries sustained by world-class volleyball players
At the index frame, the involved limb had significant/full weightbearing in 16 of the cases while moderate weight bearing of the limb was present in 5 additional cases. Table 3 also reveals the position of the knee and hip for the involved limb in the sagittal plane as well as the arms at the index frame. Attempts to perform assessment of the knee and hip positions in the frontal and transverse planes were inconsistent among reviewers and no consensus was reached.
Discussion
This is the first study to describe injury situations and injury mechanisms for acute ankle injuries sustained among world-class volleyball players. Through systematic video analysis of actual injury situations, the main findings of this study were (1) the majority of injuries occur while blocking, often landing on an opponent; (2) the attacker is overwhelmingly to blame for injuries at the net secondary to crossing the centre line and landing partially into the blocker’s court; (3) injuries during the attacking phase are often from a back-row player landing on a front-row teammate and (4) landing-related injuries mostly result from rapid inversion without any substantial plantarflexion.
Landing on another individual is the most common inciting event
Landing-related injuries during traditional volleyball play including blocking, attacking and setting accounted for nearly all of the acute ankle injuries observed in world-class players. Of these, the vast majority (90%) were the result of one individual landing on another. This is consistent with previous studies that used questionnaires, including examination of ankle sprains in Norwegian volleyball that found 87% occurred when landing on the foot of an opponent or teammate.3 9 Any interventions designed to prevent acute ankle sprains in the sport likely need to focus on minimising the risk of players landing on one another through education on typical injury situations and technical training for take-offs and landings.21
Blocking injuries mostly involve landing on another player and an attacker crossing the centre line
The act of blocking puts players more at risk than other components of the game. Blockers sustained 62.5% of ankle sprains in this study, which is consistent with previous findings that 61% of ankle injuries transpired while blocking in the top Swedish division.2 Typically, blockers are injured when landing on an opponent or teammate. When blockers land on a teammate, the injury often happens because one or both of the blockers are moving laterally during an attempt to close the block to make it difficult on the hitter. In these situations, the middle blocker was drifting laterally in all of the incidents that resulted in injuries to middle blockers or their teammates.
Plays in which the blocker landed on an opponent mostly resulted from the attacker landing under the net and partially into the blocker’s side of the court. This mainly happens if the set is tight to the net and the attacker jumps and lands under the net, but can also result from an errant jump in which the attacker simply jumped and landed too tight despite a good set.
No centre line violations, but all injuries under the net involve landings on the centre line
All the injuries involving contact with the opposition were a result of players landing on the centre line under the net. The attacking player landed on the centre line in every situation and landed partially into the opponent’s court in all but one play. FIVB rules allow a player to land with a foot partially into the opponent’s court as long as the penetrating foot maintains contact with the centre line or is directly over the centre line.22
No centre line violations were incurred by any of the players; however, a player landing on the centre line was a contributing factor in all of the situations examined. Injuries to blockers landing on opposing attackers continue to be the most common situation associated with ankle injuries at this level of the sport. One previous attempt to make the centre line rule more strict during a preseason tournament in Norway resulted in substantial disruption to the game through a significant increase in centre line violations and the rule being changed back prior to the start of the regular season.23 If players were given more time to adjust to the strict centre line rules, the number of violations may decrease. Additional consideration may be given for a rule change that makes centre line violations strict for attacking players but lenient in other scenarios where there is no/less risk of ankle injury. While it is unclear exactly what effect changes to the centre line rules would have on injury incidence, proposals to restrict contact with the centre line or opponent’s court within the conflict zone under the net should be considered.24
Attacking injuries: most commonly resulting from back-row attacks
This study is the first to describe back-row attacks as a common injury situation. In fact, two-thirds of attacking injuries resulted from a back-row attacker landing on an inattentive front-row teammate. Each of these injuries was the result of offences operating out of system. Coaches and players need to recognise these potential at-risk situations and be certain that no front-row players move into the landing path of the back-row hitter, eager to cover potential block returns.
Injuries mostly occur through inversion, with the absence of plantarflexion
The typical injury involves the ankle dorsiflexing from a plantarflexed position at initial contact towards a foot flat position on the ground. In most injury cases, inversion does not occur until the ankle is in neutral flexion with the absence of any significant plantarflexion.
This confirms recent case studies of accidental ankle sprains during laboratory cutting manoeuvres that found the ankle was in a dorsiflexed position at the moment of peak inversion.12 15 Injuries during high jumping and field hockey also report the ankle not being plantarflexed at the moment where maximal inversion occurred,13 and five cases from tennis found no significant plantarflexion component.14 Rather, inversion and internal rotation was the primary mechanism. The authors suggested that ankle sprains from jump landing in sports such as volleyball may still occur from an inversion plus plantarflexion mechanism. Our results, however, reveal that landing-related injuries in volleyball also mainly occur through inversion without any substantial plantarflexion.
Methodological considerations
This study is the first to describe injury situations and mechanisms for acute ankle injuries sustained among world-class volleyball players. The inclusion of injuries registered prospectively during the FIVB ISS has minimised the risk of selection bias of included injuries and videos. Through the use of systematic video analysis, the description of injury situations and mechanisms has been reported with improved detail and accuracy over those previously described through questionnaires which may contain recall bias from participants. While a systematic approach was used to uphold the highest levels of scientific rigour, there are several limitations which should be borne in mind when interpreting the results of this study.
One limitation is that the cases included are limited to only senior-level world-class competitions. Injury mechanisms within younger players and lower levels of adult competitors may differ. Second, injuries were only available from match play; there may be additional or other risks involved during training. Additionally, video analysis studies are dependent on the quality of the video and the number of camera views available. While most of the current videos had good quality with multiple views, there were a couple of cases in which the injury situation was easily observed but the motion of the ankle was obscured. We used a systematic approach to best determine the exact moment of injury and to ensure each reviewer evaluated the same time point, but although correspondence between reviewers was near perfect, we cannot be sure that this was when the ligament tear occurred. Also, the videos received were from television broadcasts and while this provided high-quality views from different vantage points, in the majority of cases the index frames analysed were from slow motion replays at unknown speeds. This left us with unknown time gaps between frames and the inability to perform an accuracy calculation of the proposed index frame estimates prior to eventual consensus of the final index frames by all three reviewers, as performed by Bere et al.25 Furthermore, the injury reporting forms used within the ISS do not include information relating to the specific anatomical structures involved; we therefore cannot draw conclusions on the relationship between injury mechanisms and associated structural involvement. Finally, reports of hip and knee mechanics were limited as attempts to assess their positions in the frontal and transverse planes were inconsistent among reviewers.
Conclusions
Systematic video analysis of actual injury situations revealed that the majority of injuries occur while blocking—often landing on an opponent, the attacking player is overwhelmingly to blame for injuries at the net secondary to crossing the centre line and landing partially into the opponent’s court, and injuries during the attacking phase are often from a back-row player landing on a front-row teammate. Also, landing-related injuries mostly result from rapid inversion in neutral flexion without any substantial plantarflexion.
What are the new findings?
The majority of injuries occur while blocking, often landing on an opponent
The attacker is overwhelmingly to blame for injuries at the net secondary to crossing the centre line and landing partially into the blocker’s court
Injuries during the attacking phase are often from a back-row player landing on a front-row teammate
Landing-related injuries mostly result from rapid inversion in neutral flexion without any substantial plantarflexion
How might it impact on clinical practice in the near future?
Education should be given to front-row attackers on jump technique so that they do not land under the net and into the opponent’s court regardless of the location of the set.
Education should be given to front-row players to avoid standing in the landing path of back-row attackers
Rule changes regarding a stricter centre line rule, especially for attacking players, may be considered and attempts to abolish the current centre line rule should be resisted.
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Acknowledgments
The authors thank the FIVB staff and officials for their support of the FIVB ISS and practical support in acquisition of videos.
References
Footnotes
Contributors CS, TB, RW and RB contributed to project planning and data collection. CS, JK, MAB, RW and RB performed data analysis. CS, RW and RB analysed and interpreted the data and wrote the first draft of the paper. All authors reviewed and approved the manuscript.
Funding The FIVB ISS has been established based on financial support from the FIVB. The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Norway Regional Health Authority, the International Olympic Committee, the Norwegian Olympic Committee & Confederation of Sport, and Norsk Tipping AS.
Competing interests None declared.
Ethics approval Regional Ethics Committee Midt-Norge.
Provenance and peer review Not commissioned; externally peer reviewed.