Article Text

Abstract
Objectives—To identify physical activity that is beneficial for the maintenance of bone strength with increasing age by examining the relation between bone mineral density (BMD) and chronic endurance training in men. BMD at the proximal femur, its subregions, and the lumbar spine, and serum testosterone were compared between two groups of long distance runners with more than 20 years of training experience and non-athletic controls.
Methods—Runners (n = 12) were divided into (a) high volume runners (n = 7), running 64–80 km a week, and (b) very high volume runners (n = 5), running more than 95 km a week, and compared with non-athletic male controls, exercising in non-endurance oriented activities two to four times a week. BMD (g/cm2) at the total proximal femur, femoral neck, trochanteric region, and lumbar spine was measured by dual energy x ray absorptiometry. Total testosterone (nmol/l) and free testosterone (pmol/l) in serum were measured by radioimmunoassay from single fasting blood samples.
Results—Height, weight, and age (range = 40–55 years) were not significantly different between groups. The high volume runners had significantly higher BMD at the total proximal femur (1.09 (0.17) v 0.94 (0.056)), femoral neck (0.91 (0.16) v 0.78 (0.071)), and trochanteric region (0.85 (0.14) v 0.73 (0.053)) than controls (p<0.05). The differences in BMD for the proximal femur between the very high volume runners and the other two groups were not significant. There was no difference in lumbar spine BMD, total testosterone, or free testosterone between groups. However, there was a significant negative correlation between total testosterone (r = −0.73, p<0.01) and free testosterone (r = −0.79, p<0.005) and running volume in the distance runners.
Conclusions—Long term distance running with training volumes less than 80 km a week had a positive effect on BMD of the proximal femur. With running volumes greater than 64 km a week, training was inversely related to testosterone levels, but levels remained within the normal range.
- exercise
- bone mineral density
- male athletes
- runners
- endurance training
- testosterone
Statistics from Altmetric.com
Take home message
Moderate long term distance running in the range of 64–80 km a week has a positive influence on BMD of the proximal femur, but higher volumes of running do not elicit the same benefit in middle aged men. Although testosterone levels are negatively related to training volume, they do not predict BMD in distance runners and healthy active controls.
Physical activity level is an important, modifiable influence on bone mineral density (BMD). For this reason, and given that high bone mass reduces the risk of osteoporotic fracture, it is essential to define the levels of physical activity that will optimise bone health. Mechanical loading of the skeleton has been positively associated with BMD in studies that compared male athletes from a number of different sports with less active controls.1–3
Evidence from animal4–6 and cross-sectional athlete7–8 studies indicate that both the magnitude and volume of loading influence a site specific skeletal response. The bone strains associated with distance running, a highly popular weight bearing activity, are of less magnitude but greater volume than those of high impact sports or resistance training. Although some studies comparing male distance runners with less active controls have reported higher BMD9 or bone mineral content (BMC)10 in the runners, others have found the opposite.11,12 The conflicting results may be a manifestation of the large range in age, training volume, and training years of the subjects.
Several studies reviewed elsewhere13 have documented training volume related alterations in the regulation of the hypothalamic-pituitary-gonadal axis in male endurance athletes.14,15 Chronic high mileage training in some studies has resulted in lower levels of circulating testosterone than in sedentary or less active men.16–18 There is accumulating evidence that, in runners, there may be a threshold at around 100 km a week, above which there are negative implications for testosterone regulation.13
Testosterone is an important determinant of BMD during growth and for the adult skeleton.19 Secondary osteoporosis could result from chronic suppression of testosterone levels with distance running. The relations between high and very high mileage distance running, BMD, and testosterone regulation in men have not been defined, as there have been no studies of high mileage runners with 20 year running histories. Thus we examined the relation between training volume, serum testosterone, and BMD at the proximal femur and lumbar spine in two groups of runners (high volume and very high volume) with a minimum of 20 years of consistent running training and a normally active control group.
Methods
DISTANCE RUNNERS
Twelve competitive white male distance runners were recruited from a mailing list of male masters runners over the age of 40 provided by the provincial athletic organisation in British Columbia, Canada. These runners were registered with the cross country/road running/track and field association, and had therefore competed in a race within the previous year. Fifty seven potential subjects were invited to enter the study if they met the following criteria: (a) age between 40 and 55 years; (b) training at a minimum weekly running volume of 64 km a week for at least 20 years; (c) planning to compete in a running competition of at least 10 km within the year; (d) non-smoker. Of the 18 respondents, 12 men met the selection criteria. The high volume runners (n = 7) reported a training volume of between 64 and 80 km a week, and the very high volume runners (n = 5) a volume of between 95 and 112 km a week. Subjects reported starting age of training, current and previous training volumes (km a week), and training hours in a questionnaire.
NON-ATHLETIC CONTROLS
Healthy white men were recruited and matched for age and weight with the distance runners. Inclusion criteria were (a) age between 40 and 55 years; (b) non-smoker; (c) participating in non-endurance type activities two to four times a week; (d) weight between 61 and 87 kg. Twelve of 16 respondents met the entry criteria and were included.
The study was approved by the University of British Columbia clinical screening committee for research and other studies involving human subjects. All subjects provided written consent and completed the study.
BONE DENSITOMETRY
BMD of the proximal femur (total, femoral neck, trochanteric region) and the lumbar spine (L1–L4) was measured by dual energy x ray absorptiometry (QDR 4500; Hologic Inc, Waltham, Massachusetts, USA). All scans were performed by the same registered technician. Proximal femur scans were performed on the non-dominant side. The in vitro precision value for our instrument was 0.5% at the lumbar spine.
HORMONE ANALYSIS
Subjects reported to the university medical centre between 0700 and 0900 after 12 hours of fasting and 36 hours without strenuous exercise. A single 10 ml blood sample was collected from each subject by the same doctor and clotted at room temperature. Samples were then centrifuged at 3200 rpm and 4°C. Serum was separated from the rest of the sample and stored at −70°C to await batch analysis. Hormone analyses were performed on serum, using competitive binding radioimmunoassays. Total testosterone was analysed using the ACS: 180 testosterone assay (Chiron Diagnostics, East Walpole, Massachusetts, USA). Sensitivity for this assay falls between testosterone concentrations of 0.35 and 52.0 nmol/l, with a reported precision of 6.5% (coefficient of variation) within the normal physiological range for total testosterone.20 Free testosterone in serum was assessed using the Coat-A-Count free testosterone radioimmunoassay (Diagnostics Products, Los Angeles, California, USA). The kit is sensitive for free testosterone values ranging from 1.9 to 173 pmol/l, and can detect as little as 0.52 pmol/l free testosterone. Precision values (coefficient of variation) of 3.8% for within run tests and 4.2% for run to run tests have been reported.21
ANTHROPOMETRIC MEASURES
Height (in m, to the nearest 0.005 m), weight in light clothing (in kg, to the nearest 0.1 kg), and sum of seven skinfolds (in mm, to the nearest 0.1 mm) including triceps, biceps, subscapular, suprailiac, abdominal, thigh, and medial calf were measured according to Canadian Physical Activity, Fitness and Lifestyle Appraisal (CPAFLA) guidelines.22 Body mass index (BMI, weight/height2) was calculated.
ASSESSMENT OF NUTRIENT INTAKE
Subjects completed a three day dietary record, which was analysed by the Foodsmart computerised dietary analysis system (Sasquatch Software, North Vancouver, British Columbia, Canada). Average daily total energy (kcal) and calcium (mg) intakes were calculated and compared.
STATISTICAL ANALYSIS
Differences between very high volume, high volume, and control groups were determined by one way analysis of variance, followed by Tukey's HSD post hoc analysis. Statistical significance was set at p<0.05. We examined the relation between BMD, total/free testosterone, and other descriptive variables using Pearson's product-moment correlation coefficients.
Results
SUBJECT CHARACTERISTICS
Table 1 summarises the physical characteristics, dietary intake, and general training characteristics of the subjects. Age, height, weight, and BMI did not differ significantly between groups. The sum of seven skinfolds was significantly higher in the control group (p<0.05). The minimum competitive distance in runners was 3000 m steeplechase (n = 1). All other runners had competed in 10 km events, nine had competed in marathons, and two in ultramarathons (100 km). All runners cross trained in other activities including cycling, swimming, and/or resistance training. Runners performed less than two hours of resistance training a week. Controls reported walking, hiking, resistance training, cycling, golfing, and tennis, but did not perform any endurance training. Nine control subjects resistance trained for two to four hours a week. Average daily calcium and energy intakes were not significantly different between groups (table 1).
Physical and training characteristics of very high volume runners, high volume runners, and controls
BMD
High volume runners had significantly higher mean BMD than controls at the total proximal femur (1.09 (0.17) v 0.94 (0.056)), femoral neck (0.91 (0.16) v 0.78 (0.071)), and trochanteric regions (0.85 (0.14) v 0.73 (0.053)) (all p<0.05). The difference between high volume runners and controls at the lumbar spine was not significant (1.04 (0.16) v 0.92 (0.095)). The mean BMD for the very high volume runners was not significantly different from that of controls or high volume runners at any site: total proximal femur (0.98 (0.11)), femoral neck (0.81 (0.074)), trochanteric region (0.76 (0.093)), and lumbar spine (0.90 (0.070)) (fig 1).
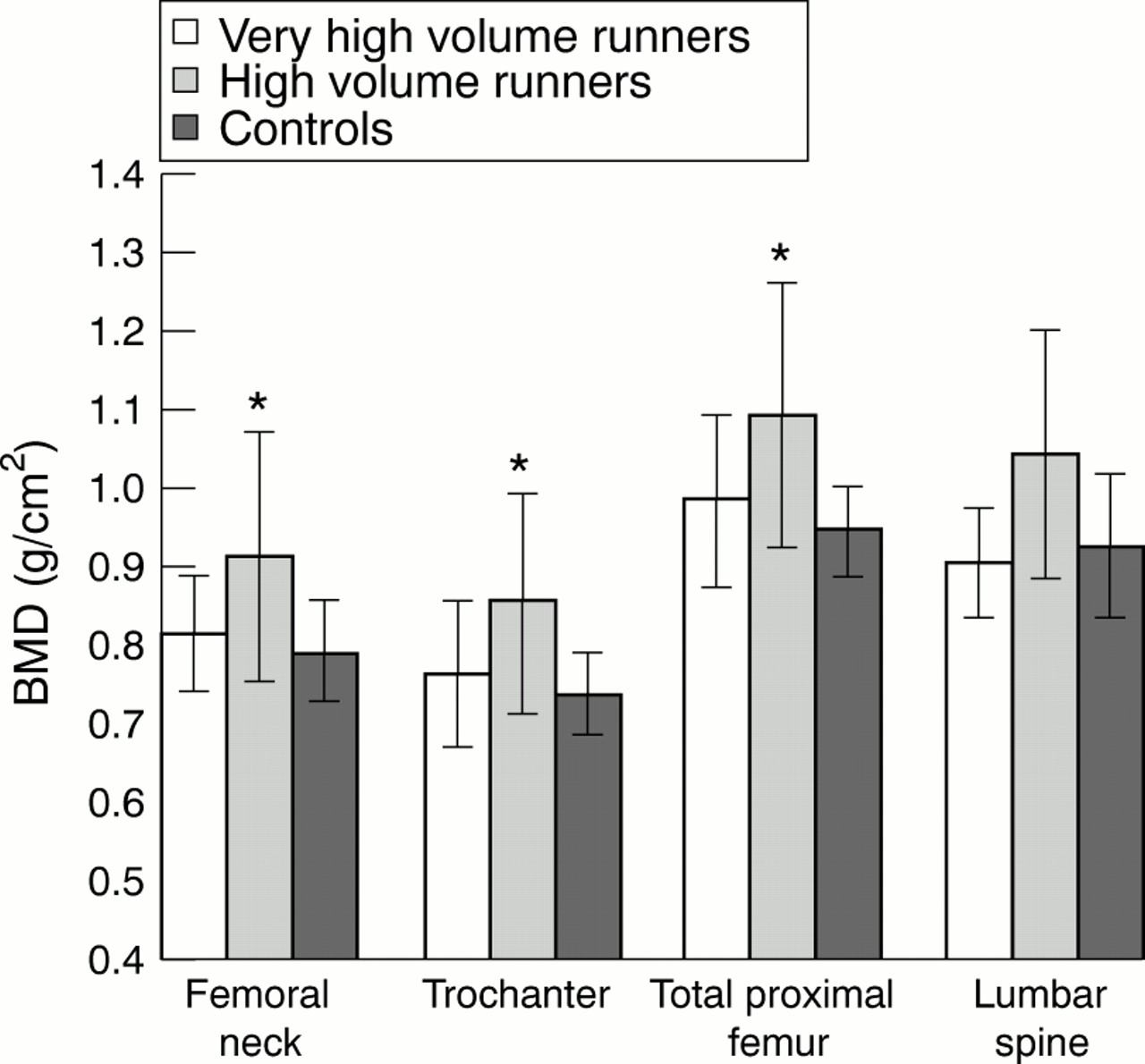
Mean bone mineral density (BMD) for very high volume runners, high volume runners, and controls. *Significantly higher than controls, p<0.05.
At the femoral neck, trochanter, and total proximal femur, all three group means were within 1 standard deviation of same age BMD z scores provided by the manufacturer of the dual energy x ray absorptiometer (Hologic Inc). At the lumbar spine, all three group means were within 1.3 standard deviations of the reference sample (very high volume, −1.3; high volume, −0.12; controls, −1.3).
HORMONE ANALYSES
There were no significant differences in either total testosterone or free testosterone between groups. The very high volume runners had the lowest mean total and free testosterone when compared with high volume runners and controls (not significant). In all three groups, both total and free testosterone were within the normal range for this population (table 2). The mean free testosterone value for the very high volume runners (54.4 (7.9) pmol/l) fell just above the lower limit for normal.
Mean total testosterone and free testosterone for very high volume runners, high volume runners, and controls
In the runners, simple correlation showed significant negative associations between weekly training volume and total testosterone (r = −0.73, p<0.01), and weekly training volume and free testosterone (r = −0.79, p<0.005; fig 2). The correlations between free/total testosterone and BMD at all sites were not significant (r values ranged from 0.03 to 0.16, p>0.45 for all relations).

{kind=link}
{kind=link}
Scatterplot of free testosterone levels (pmol/l) v running volume for 12 distance runners. r = −0.79, p<0.005.
Discussion
This study is the first to evaluate regional BMD in 40–55 year old distance runners who had trained and competed consistently for a minimum of 20 years. Its design allowed us to observe athletes whose training level was very consistent for nearly half of their lives. High volume distance running, between 64 and 80 km a week, was positively associated with BMD at the mechanically loaded proximal femur, but not at the lumbar spine. BMD of very high volume runners who ran more than 95 km a week for over 20 years did not differ from controls. Although lower testosterone levels were significantly related to higher training volumes, the hormone levels did not explain the between group differences in BMD.
PROXIMAL FEMUR
Training volume (high volume runners v controls)
Our observation of higher proximal femur BMD in the high volume runners is consistent with two other cross sectional studies that examined BMD of the lower extremity in younger runners performing similar training volumes. About 10% higher proximal femur BMD was observed in adult male runners (mean age 32 years) averaging about 70 km a week than in age matched controls.10 Femur (proximal femoral neck to knee joint) BMD in male endurance track athletes between the ages of 17 and 26, training an average of 10.9 (5.1) hours a week, was 6.75% higher than in sedentary controls.8 However, MacDougall et al23 reported significantly higher lower leg (tibia + fibula) BMD in runners (aged 20–45) not exceeding 32 km a week compared with two control groups (active and sedentary men). There was a trend towards lower BMD in runners training between 32 and 88 km a week, and the BMD for this group was higher than that of the sedentary controls, only.
Training volume (very high volume runners v controls)
Our finding that the proximal femur BMD of the very high volume runners (>95 km a week) did not differ significantly from that of the control group is similar to the report by MacDougall et al23 on runners training over 100 km a week. Hetland et al11 reported lower BMC at the trochanteric region in runners training at least 100 km a week than in non-running active controls. However, the BMC of these runners was not lower than that of controls at the femoral neck, an area that responds to compressive loading to a greater extent than the trochanter.24 In their study, the negative association between training volume and trochanteric BMC remained significant when the model was corrected for body size.11
Training volume (threshold)
The results of this study, and others that evaluated proximal femur BMD in distance runners11,23 training at high (up to about 90 km a week) compared with very high (>90 km a week) volumes suggest that a volume threshold exists. Animal experiments also suggest that above a certain load frequency no further increases are observed in BMC and BMD.5,6 In the classic studies by Lanyon,5 36 loading cycles a day were as effective as 360 or 1800 in increasing BMC in turkey ulnae. Umemura and colleagues6 showed that five jumps a day were as effective as 40–100 jumps in increasing BMC. The present study suggests that a positive training response is obtained when the training volume is below 95 km a week.
Influence of age/training years
Age25 and, possibly, years of continued training26 may be as important as training volume for proximal femur BMD in older athletes, underlining the importance of considering all three of these variables. The strengths of this study are that, firstly, subjects had maintained consistent training volumes for a minimum of 20 years, and secondly, subjects were all aged between 40 and 55 years. Limited comparisons can be made between our study and others measuring more widespread age groups of male runners, whose training volume and training years vary considerably.9,27
In both their five28 and nine9 year longitudinal studies, Lane et al suggested that training volume must be maintained to keep the higher BMD noted in aging runners compared with controls. Although both runners and controls lost bone mineral over time, the loss was greatest in those runners who decreased their running volumes substantially.28 Runners in our study maintained high training volumes for more than 20 years, and this may have contributed to the observed differences in BMD.
The net gain of bone that results from modelling in response to high mechanical loads or strain occurs primarily during growth,29,30 and “starting age” of training can substantially influence peak BMC.31 Five of the seven high volume runners had commenced vigorous training before the age of 18, while only one of the very high volume runners had done so before 18. Thus the high volume runners may have had a higher BMD when they reached adulthood. The design of this study did not permit us to evaluate the specific influence of childhood activity on adult bone status.
LUMBAR SPINE
We observed no difference in lumbar spine BMD among groups, and this is consistent with the report from Goodpaster and colleagues.27 Their group found no difference in BMD between middle aged, previously elite (previously training between 80 and 150 km a week) distance runners currently training at various levels compared with normative values. However, others have found lower vertebral bone mineral in young adult runners training over about 92 km a week, as compared with controls.11,12 One study suggested a positive association between low volumes of distance running, about 43 km a week, and lumbar spine BMD.9 Potential mechanisms that may explain our results relate to the biomechanical forces associated with running and the endocrine regulation of bone mass.
Biomechanics of loading: site specificity
We observed the greatest bone benefit at the primary weight bearing sites—that is, lower limb—which is consistent with the mechanostat theory.32 Jogging elicits peak forces at the hip in the range of five to six times body weight,33 but these forces are attenuated as they propagate into the lumbar spine.34 Bennell et al8 reported diminishing BMD differences between track athletes and controls at skeletal sites at increasing distances from the foot. There were no differences at the lumbar spine.8 Furthermore, BMD increases are more likely to occur under unusual strains of uneven distribution, than under the repetitive low amplitude strains associated with running or other daily physical activities.35
Our controls were recreationally active healthy men, who participated in weight bearing non-endurance exercise at least twice a week, and not purely sedentary men. This may have tended to equalise our groups in terms of loading at the lumbar spine and thus limit BMD differences at this site. Although the controls performed less activity overall than the runners, they participated more often in activities such as weight lifting, tennis, and heavy yard work. It is likely that these exercises represented unique stresses to the skeleton, which could load the lumbar spine as much as the repetitive reaction forces induced in distance running.36
TESTOSTERONE
In our study, there was a negative correlation between weekly running volume and both total and free testosterone; however, the within group variances were high. This, and the relatively small sample size, may partially explain the non-significant differences in both free and total testosterone between groups. However, the lowest absolute value for both measures belonged to the very high volume runners. This group had a mean free testosterone level just above the lower limit of the physiological normal range. In several previous studies, distance runners (training more than 95 km a week) had lower resting testosterone levels than less active men.15–17 Future studies with serial blood sampling over time may have greater power to detect differences in testosterone levels between groups of distance runners.
TESTOSTERONE/BONE RELATION
In our study and in others,14–18,37 the reported testosterone levels in distance runners fell within the normal healthy range. In two studies, BMD of chronically hypogonadal men (with testosterone levels below the normal range, as in Klinefelter's syndrome and hypogonadotropic hypogonadism) was significantly lower than that of men who had normal testosterone levels.38,39 Although researchers report differences in testosterone levels when comparing less active controls with distance runners,15–17 the testosterone-bone relation remains clinically insignificant when normal levels of testosterone are maintained.
CLINICAL IMPLICATIONS
-
Both high and very high volume running are associated with normal BMD.
-
High (but not very high) running volumes are associated with higher BMD than that of non-athletic controls, thereby conferring a slightly decreased risk of osteoporotic fracture.
-
Although testosterone levels were negatively associated with training volume, most fell within the normal range and were not related to BMD.
CONCLUSIONS
In this study of 40–55 year old men, running 64–80 km a week was associated with proximal femur BMD that exceeded that of active controls. However, running more than 95 km a week was associated with BMD equivalent to active controls. Although we observed a negative association between free testosterone and training volume in this study of healthy male adults, this did not explain the differences in BMD between groups.
Acknowledgments
This project was funded by The Vancouver Medical Services Foundation (grant no BCM97-0137). We thank the staff at Fairmont Bone Density as well as the technicians at Clinical Chemistry, Vancouver Hospital for analysing the blood samples.
Contributors: K M initiated the study, formulated the initial hypotheses, and coordinated all aspects of data collection, analysis, and writing of the paper. J T refined the hypotheses, assisted in subject recruitment, collected blood samples for hormone analysis, and edited initial manuscripts. H Mc directed the analysis and discussion of BMD measurements, and worked closely with K M in the writing of the paper. H Mc is the guarantor for this study. K K stimulated discussion of the results and edited the paper extensively.
Take home message
Moderate long term distance running in the range of 64–80 km a week has a positive influence on BMD of the proximal femur, but higher volumes of running do not elicit the same benefit in middle aged men. Although testosterone levels are negatively related to training volume, they do not predict BMD in distance runners and healthy active controls.
References
Linked Articles
- Editorial