Article Text

Abstract
Background Lateral ankle sprains are common and can have detrimental consequences to the athlete. Joint mobilisation/manipulation may limit these outcomes.
Objective Systematically summarise the effectiveness of manual joint techniques in treatment of lateral ankle sprains.
Methods This review employed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A computer-assisted literature search of MEDLINE, CINHAL, EMBASE, OVID and Physiotherapy Evidence Database (PEDro) (January 1966 to March 2013) was used with the following keywords alone and in combination ‘ankle’, ‘sprain’, ‘injuries’, 'lateral’, ‘manual therapy’, and ‘joint mobilisation’. The methodological quality of individual studies was assessed using the PEDro scale.
Results After screening of titles, abstracts and full articles, eight articles were kept for examination. Three articles achieved a score of 10 of 11 total points; one achieved a score of 9; two articles scored 8; one article scored a 7 and the remaining article scored a 5. Three articles examined joint techniques for acute sprains and the remainder examined subacute/chronic ankle sprains. Outcome measures included were pain level, ankle range of motion, swelling, functional score, stabilometry and gait parameters. The majority of the articles only assessed these outcome measures immediately after treatment. No detrimental effects from the joint techniques were revealed in any of the studies reviewed.
Conclusions For acute ankle sprains, manual joint mobilisation diminished pain and increased dorsiflexion range of motion. For treatment of subacute/chronic lateral ankle sprains, these techniques improved ankle range-of-motion, decreased pain and improved function.
- Ankle Injuries
- Intervention Effectiveness
- Lower Extremity Injuries
- Physiotherapy
- Sports Rehabilitation Programs
Statistics from Altmetric.com
- Ankle Injuries
- Intervention Effectiveness
- Lower Extremity Injuries
- Physiotherapy
- Sports Rehabilitation Programs
Introduction
Lateral ankle sprains are common in active people and the ankle is one of the most commonly injured joints in sports.1 ,2 A recent systematic review demonstrated that the ankle was the most common site of injury in 24 of 70 sports examined, accounting for 10–30% of all sport injuries.2 In addition, 19% of sports injuries presenting to emergency rooms were ankle injuries.3 Ankle sprains result in a substantial number of missed work days4 and participation in sports activity.5
The majority of these sprains are a result of forced ankle inversion and plantarflexion. Lateral ankle sprains are also referred to as inversion ankle sprains or occasionally as supination ankle sprains. The severity of ankle sprains can vary widely. Ankle injuries are common with athletic activities that require jumping, running and/or explosive lateral cutting.2 ,6
An acute ankle sprain results in injury to the lateral ligaments,7 pain, swelling and limitation of movement.7 Subsequent short-term and long-term losses of joint range of motion (ROM), specifically dorsiflexion, and muscle strength lead to functional and sport-specific limitations. A concern for healthcare providers is the potential progression of acute ankle sprains to chronic problems, including arthritic changes in the talocrural joint.8 Symptoms have been shown to persist for 6 weeks to 18 months after a lateral ankle sprain in 55–72% of patients.9–11
Dorsiflexion limitations exist in the acute and subacute stages.12 Denegar et al13 found restricted posterior talar glide in athletes 12 weeks after acute ankle sprain. This loss of mobility of the talus can lead to inadequate ROM resulting in altered biomechanics and dysfunction during gait.14 Biomechanically limited ankle dorsiflexion places the talus in a more anterior position during weight-bearing, increasing the load on the anterior talofibular ligament, leaving the patient susceptible to repetitive ankle sprains.15 Chronic ankle instability may be caused by mechanical instability, functional instability or a combination of both.16
Previous studies have demonstrated that manual therapy techniques are beneficial in restoring or improving dorsiflexion,9 ,13 ,17 posterior talar glide,13 ,17 stride speed and step length9 and force distribution of the foot.18 Whitman et al19 documented favourable clinical outcomes in approximately 75% of patients postacute ankle sprain following two sessions of mobilisation and manipulation to the rearfoot and proximal tibiofibular joint.
A number of systematic reviews have investigated the effectiveness of various treatments after ankle sprains with mixed results.20–22 More recent studies have demonstrated moderate evidence that manual therapy may be beneficial in the treatment of patients with ankle sprains.18 ,23–25 The purpose of this systematic review was to evaluate and update the clinical evidence specifically based on the effectiveness of manual joint mobilisation/manipulation in the treatment of lateral ankle sprains.
Methods
Study design
The design of this systematic review was developed using the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The PRISMA statement includes a 27-item checklist that is designed to be used as a basis for reporting systematic review of randomised trials.26
Search strategy
Identification of studies
The systematic, computerised literature search was performed by one reviewer (JKL) and encompassed five databases including MEDLINE, CINAHL, EMBASE, Physiotherapy Evidence Database (PEDro) and OVID databases. The following search terms alone and in combinations were used: ‘ankle’, ‘sprain’, ‘injuries’, 'lateral’, ‘manual therapy’ and ‘joint mobilisation’. Additionally, the reference lists of all selected publications were screened to retrieve relevant publications that were not identified in the computerised search. The search was concluded on 1 March 2013.
Full-text randomised controlled trials published in English and found in peer-reviewed journals were considered for the study. The study needed to include humans with a lateral ankle sprain. The time after the injury was identified as acute, subacute or chronic. The selection of intervention included joint mobilisation or manipulation of the distal tibiofibular, talocrural, subtalar joint or midfoot. The intervention had to be compared with a control group. At least one of the following outcome measures had to be used for inclusion in this study: ankle joint ROM, pain level, swelling and/or some type of functional outcome. Outcome measurement follow-up times were defined as either short term (<3 months), medium term (3–6 months) or long term (>6 months). The excluded articles were those that investigated ankle injuries other than lateral ankle sprains such as high ankle sprains or fractures and included other interventions in addition to manual joint techniques.
Selection of studies
The selection of studies was a two-stage process. For the first stage, titles of all identified citations were independently evaluated by two reviewers (JKL and MPR). The article was included in this first screen if the title identified the use of manual therapy for the treatment of an ankle sprain. All articles that were identified as meeting the search criteria were included in the next stage of the review, which was to review the article abstracts. If there was insufficient information from the abstract to establish eligibility, the full-text article was retrieved and read independently by both reviewers. Any disagreement was resolved by consensus.
Quality assessment of studies
The methodological quality of individual studies was assessed using the PEDro scale.27 Two reviewers (MPR, JS) independently assessed the quality of the studies. Disagreement or ambiguous issues were resolved by consensus discussion with a third reviewer (JKL).
PEDro uses 11 criteria, and reviewed studies were awarded one point for each criterion that was clearly satisfied. Criteria included (1) eligibility criteria reported; (2) random assignment; (3) concealed allocation; (4) groups similar at baseline regarding most important prognostic indicator; (5) blinding of participants; (6) blinding of therapists who administered the therapy; (7) blinding of assessors who measured key outcome; (8) measures of at least one key outcome were obtained from more than 85% of initial participants; (9) all participants received treatment or control condition as allocated; (10) results of between-group statistical comparisons are reported and (11) study provides both point measures and measures of variability for at least one key outcome.27 The reviewing investigator assigned one point to each factor met, which generated a potential maximum value of 11 points. This information is displayed in table 1.
PEDro quality assessment of individual trials
Results
Selection of studies
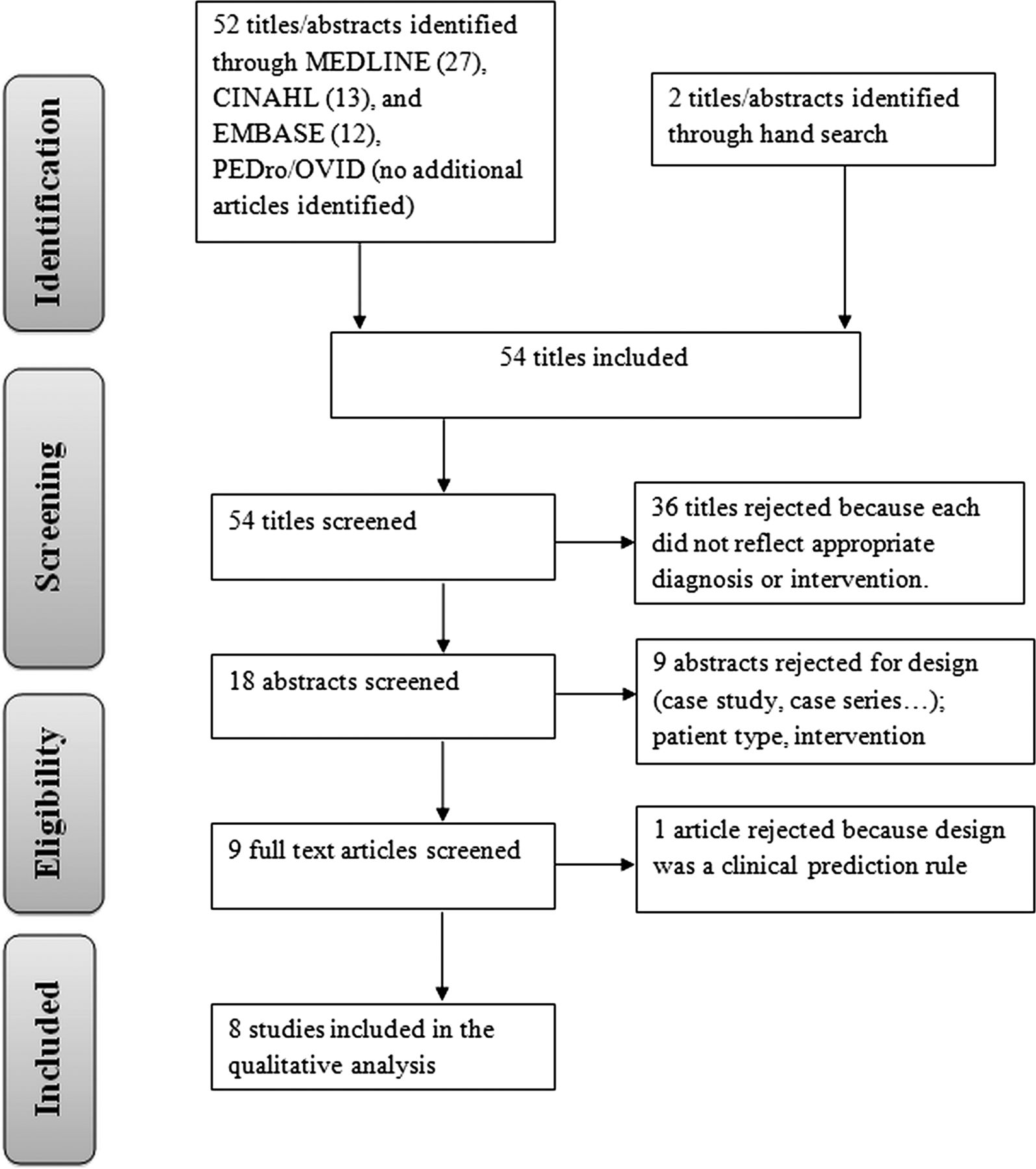
Fifty-four titles were identified through database and reference searches. Eighteen abstracts were then assessed for eligibility for inclusion, resulting in nine appropriate studies. After further review of full text, one article was designed as a clinical prediction rule and therefore was excluded leaving eight articles9 ,18 ,23–25 ,28–30 (244 participants) to review. Figure 1 shows the process of study selection and the number of studies excluded at each stage, with reasons for exclusion. Within these eight articles, all participants had a history of lateral ankle sprain, three studies9 ,23 ,29 involved participants with acute ankle sprains (110 participants) and the remaining five studies18 ,24 ,25 ,28 ,30 included participants with subacute or chronic ankle sprains (134 participants). The majority of studies included a separate control group for their experiments; in three studies24 ,25 ,28 participants served as their own control. The number of participants in the reviewed studies ranged from 1325 to 55.29 Follow-up ranged from immediately following treatment9 ,18 ,24 ,25 ,28–30 to 1 month.30 Table 2 describes the population, intervention, outcome measures and results of the included studies.
Description of studies included in review
{kind=link}
Flow diagram for study inclusion.
Quality of studies
The scores on each of the 11 criteria and total scores for each study are presented in table 1. The overall score rating for each of the eight articles had 50% agreement. The difference in overall scoring was one point for three articles and two points for one article. For the individual items of the PEDro, items 1, 2, 3, 5, 7, 9, 10 and 11 had 100% agreement, item 6 had 86% agreement, and items 4 and 8 had 75% agreement. Disagreement was resolved by consensus.
Three articles24 ,25 ,28 achieved a score of 10 of 11 total points; one23 achieved a score of 9, one article9 scored 8, one article30 scored a 7, one article29 scored a 6 and the remaining article18 scored a 5. The nature of the studies made it difficult for blinded application of the manual therapy intervention. Half of the eight articles24 ,25 ,28 ,29 had groups that were similar at baseline for the primary outcome. Long-term follow-up was lacking in the majority of the studies.9 ,18 ,24 ,25 ,28–30
Effect of manual joint techniques for acute lateral ankle sprains
Three articles9 ,23 ,29 investigated the effect of manual therapy for an acute lateral ankle sprain. These articles scored a six or better on the PEDro scale. Green et al9 utilised an anteroposterior (AP) mobilisation of the talus over a 2-week period along with standard care and found an increase in pain-free dorsiflexion ROM by day 8–10 postinjury. This result was superior over a group that only received the standard care of rest, ice, compression and elevation (RICE). Additionally, the intervention group showed an increase in stride speed as compared with the control group.
In a second study using the same talar AP manual technique, Cosby et al23 found that participants had an improvement in pain perception compared with a control group following a single bout of the intervention. No significant improvement in dorsiflexion ROM or self-perceived function was found between groups.
Eisenhart et al29 assessed oedema, sagittal plane ROM and pain following a variety of osteopathic techniques on participants following ankle sprain. These techniques were based on the individual participant's discovered restrictions and included manipulation of the distal fibula and/or cuboid and soft tissue techniques (strain/counterstrain, muscle energy, lymphatic drainage). The experimental group had significant reduction in pain and swelling immediately following a single treatment session. At 1-week follow-up, the experimental group had statistically less difference between involved/non-involved ankles for sagittal plane ROM than the control group.
Effect of manual joint techniques for subacute/chronic lateral ankle sprains
The remaining five articles18 ,24 ,25 ,28 ,30 investigated manual joint mobilisation/manipulation on individuals with a subacute or chronic lateral ankle sprain. One high-level study by Yeo and Wright25 investigated the changes in pressure pain threshold (PPT), ankle ROM and performance on a battery of functional tests following a Maitland AP talar mobilisation. There were significant improvements in the ankle dorsiflexion ROM and PPT during the treatment condition. However, no significant improvement was observed for the other functional measures.
Two high-level studies24 ,28 used a Mulligan mobilisation with movement (MWM) technique which involved the clinician applying an AP mobilisation to the talus while the standing participant actively dorsiflexed. In both studies, an improvement in ankle dorsiflexion ROM was found preapplication to postapplication with one session of Mulligan's technique. No change in pain sensitivity was found following the joint mobilisation technique.28
Two studies utilised thrust manipulation interventions. A study by Pellow and Brantingham30 studied the effect of a talocrural distraction manipulation on the dorsiflexion ROM, pain and function. A positive effect on the dorsiflexion ROM, pain and functional score resulted at the 1-month follow-up. The lowest-rated study18 (5/11) also used a talocrural distraction technique along with an AP talar manipulation and investigated the effect of these techniques on the stability of the foot. These researchers found a significant change in foot area in the treatment group indicating greater stability.
Discussion
This systematic review is the first in over 5 years to look at the effect of manual joint therapy following a lateral ankle sprain, and the only one to investigate the effects of manual therapy as a sole intervention. Two previous systematic reviews that investigated treatment for lateral ankle sprains included other interventions such as exercise and modalities.21 ,22 van der Wees et al21 concluded from their systematic review that included four articles on mobilisation that manual mobilisation has an (initial) effect on dorsiflexion ROM, but the clinical relevance of these findings may be limited. Bleakley et al's review included two of the same studies from van der Wees et al.21 Our review, including four additional studies,18 ,23–25 shows moderate evidence that manual techniques, applied in the acute phases of injury are effective at increasing ankle dorsiflexion ROM.
Owing to the lack of studies focusing solely on manual therapy, we included articles that studied participants with either acute or subacute/chronic sprains. The joint techniques investigated in the included studies targeted the talocrural joint and the potential faulty joint position of the talus that may occur following a lateral ankle sprain. Denegar et al13 found that restricted posterior talar glide commonly limits sagittal plane ankle ROM after an ankle injury. This effect is often long lasting, with observations up to 6 months.13 There is evidence that such persistent restriction in talar gliding, can result in long-term ankle issues.31 ,32
Effect of manual joint techniques for acute
Two9 ,23 of the three9 ,23 ,29 articles that investigated manual joint mobilisation/manipulation for acute sprains used an AP talocrural mobilisation. In the study by Green et al,9 the addition of manual therapy increased dorsiflexion ROM and self-reported function sooner than the control group receiving RICE. In contrast to Green et al9 study, Cosby et al23 did not find a significant difference between groups in improvement in dorsiflexion ROM and self-perceived function, but did find a decline in pain perception. The study design developed by Cosby et al23 utilised only one treatment bout, possibly accounting for the main differences in results between the two studies.
In the third study, Eisenhart et al29 provided a single treatment of high-velocity thrust techniques tailored to the need of the participant's restrictions. Pain level and swelling decreased immediately and at the 1-week follow-up. Range-of-motion improvements were greater in the intervention group as compared with RICE alone.
It is likely that manual mobilisation has an initial pain altering effect after ankle sprains, but not a mechanical effect. Initial effects of manual mobilisation after an ankle sprain are more likely attributed to pain alteration than true mechanical effects. For significant improvement in ROM, more than one bout of mobilisation therapy, use of manipulation or use of mobilisation/manipulation combined with exercise may be necessary.
Effect of manual joint techniques for subacute/chronic
During the subacute and chronic stage of healing, pain and swelling are typically diminishing, allowing for improved function. During this phase, it might be expected that joint mobilisation techniques would have a more pronounced effect on joint mechanics than pain reduction.
Manual joint techniques, in general, have demonstrated transient biomechanical effects in studies quantifying ROM,33–,36 without lasting positional changes.37 ,38 Manual therapy applied to ankle sprains is likely to respond most favourably to manual therapy followed by exercise intervention to improve ROM as suggested by previous findings21 and similar findings in studies investigating other joints.39–42
Five articles18 ,24 ,25 ,28 ,30 were reviewed for the effect of manual joint mobilisation/manipulation that were applied during the subacute or chronic stage of a lateral ankle sprain. Two articles24 ,28 utilised MWM. Collins et al28 were able to demonstrate a significant improvement in immediate ankle dorsiflexion ROM but no hypoalgesic effect on PPT despite the fact that participants exhibited reduced PPT in the affected ankle as compared with the contralateral ankle. Although the article by Reid et al24 scored well using the PEDro scale, the results are similar to Collins et al28 demonstrating that MWM provides an immediate improvement in ankle dorsiflexion ROM. Further research is needed to analyse the long-term effect of MWM on lateral ankle sprains.
Yeo and Wright25 used the AP talar mobilisation, comparable to Green et al9 and Cosby et al23 but with a participant population that had a subacute lateral ankle sprain. Similar to a number of studies, Yeo and Wright 25 demonstrated that mobilisation of the ankle joint results in an improvement in ankle dorsiflexion ROM. In contrast to Collins et al28 but similar to Cosby et al23 Yeo and Wright25 found that their mobilisation technique produced an initial hypoalgesic effect. One may theorise that the non-weight-bearing position of the AP talar mobilisation may allow an environment for pain reduction due to decreased joint compressive forces.
The two final articles18 ,30 used some type of thrust manoeuvre on their participants with lateral ankle sprains. Pellow and Brantingham30 used a talocrural distraction manipulation and treated participants up to eight times, depending on their restrictions. Of the articles reviewed, this was the only one with a longer follow-up time (1 month). The researchers found that at 1 month, the group treated with the manipulation had improved pain level, dorsiflexion ROM and function. The small participant pool is one limitation of this study. The researchers in the last article reviewed18 used stabilometry as an outcome measure. Stability of the foot/ankle complex is important to achieve following a lateral ankle sprain to help with return to function and prevention of reoccurrence. Lopez-Rodriguez et al18 found that the group treated with manipulation had improved foot area distribution, which one would think would help with stability. The authors conclude that this change in load distribution is accompanied by proprioceptive changes, although this was not measured.
Limitations
Limitations of this review include difficulty in comparison of the eight studied articles due to the heterogeneity of techniques utilised in the studies, limited follow-up time (longest follow-up was 1 month) and the included studies only investigated immediate treatment effects. Additionally, all studies included young adults <32 years which may limit the generalisability to older populations. Lastly, none of the studies investigated the mechanism of how the joint manual techniques worked.
Conclusions
Eight studies were analysed for this systematic review on manual joint mobilisation/manipulation for lateral ankle sprains. Manual joint mobilisation appears to help to diminish pain, at least temporarily, for participants with an acute ankle sprain. Repeated bouts of manual mobilisation or manipulation is likely to have an (initial) effect on increasing dorsiflexion ROM, but the clinical relevance of these findings is unknown.
For treatment of subacute/chronic lateral ankle sprains, some form of joint manual therapy appears to help with ankle ROM, especially dorsiflexion and pain reduction. Function, at least for the short term, was also improved. No detrimental effects were revealed. Future studies that include a larger sample size and a longer follow-up period would more clearly elucidate the true benefit of these techniques, as well as their potential mechanisms.
Limited follow-up time-frame in the studies investigated in our review does not allow us to extrapolate the long-term benefits of these techniques. Additionally, mechanisms by which joint mobilisations influence these changes warrant further investigation.
What this study adds
-
This is the first study investigating joint mobilisation/manipulation as an isolated intervention for the treatment of acute and subacute/chronic ankle sprains.
-
Joint mobilisation/manipulation techniques acutely improve ankle dorsiflexion ROM and pain in all investigated groups, as well as improved function in the subacute/chronic participants.
-
The application of manual joint mobilisation/manipulation to appropriate participants presenting with acute and subacute/chronic ankle sprains appears to result in no detrimental effects.
References
Footnotes
-
Contributors JKL and MPR performed the literature search. MPR and JS graded the articles for the systematic review. JKL, MPR and JS wrote the article. JKL is the guarantor.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The data utilised for this review are present in the article.