Article Text

Abstract
Background Ankle sprains are highly prevalent with high risk of recurrence. Consequently, there are a significant number of research reports examining strategies for treating and preventing acute and recurrent sprains (otherwise known as chronic ankle instability (CAI)), with a coinciding proliferation of review articles summarising these reports.
Objective To provide a systematic overview of the systematic reviews evaluating treatment strategies for acute ankle sprain and CAI.
Design Overview of intervention systematic reviews.
Participants Individuals with acute ankle sprain/CAI.
Main outcome measurements The primary outcomes were injury/reinjury incidence and function.
Results 46 papers were included in this systematic review. The reviews had a mean score of 6.5/11 on the AMSTAR quality assessment tool. There was strong evidence for bracing and moderate evidence for neuromuscular training in preventing recurrence of an ankle sprain. For the combined outcomes of pain, swelling and function after an acute sprain, there was strong evidence for non-steroidal anti-inflammatory drugs and early mobilisation, with moderate evidence supporting exercise and manual therapy techniques. There was conflicting evidence regarding the efficacy of surgery and acupuncture for the treatment of acute ankle sprains. There was insufficient evidence to support the use of ultrasound in the treatment of acute ankle sprains.
Conclusions For the treatment of acute ankle sprain, there is strong evidence for non-steroidal anti-inflammatory drugs and early mobilisation, with moderate evidence supporting exercise and manual therapy techniques, for pain, swelling and function. Exercise therapy and bracing are supported in the prevention of CAI.
- Ankle
- Injury
- Injury prevention
- Chronic
- Sprain
Statistics from Altmetric.com
Introduction
The incidence of ankle sprain is high, posing a significant risk for participants of a wide range of activity types and sports.1 Ankle sprain is associated with significant socioeconomic cost in addition to the acute debilitating symptoms (which include pain, swelling and impaired function); each year, over two million ankle sprains are treated in emergency departments in the US and UK.2–5 The long-term prognosis of acute ankle sprain is poor, with a high proportion of patients (up to 70%) reporting persistent residual symptoms and injury recurrence.6 ,7 ‘Chronic ankle instability’ (CAI) is the encompassing term used to describe the chronic symptoms that may develop following an acute ankle sprain, with injury recurrence at the epicentre of the chronic paradigm.8
There is an abundance of literature evaluating treatment strategies for acute ankle sprains and/or CAI. In accordance with this, a large number of systematic reviews have emerged to combine these studies’ findings to synthesise and extract the best evidence for treatment guidelines. However, there are now such a large number of systematic reviews that identification, appraisal and consideration of each individual paper is not feasible for practitioners. This issue is further compounded by the probability that these reviews vary in quality and scope (with several reviews for one prevention/treatment type) and their inclusion of papers with a high degree of overlap in the injury target (acute ankle sprain/CAI). Thus, there is a need to collate this evidence in a non-biased, systematic manner to ascertain evidence-based recommendations for the treatment of acute ankle sprain and CAI.
The aim of this paper was to provide a systematic overview of the systematic reviews evaluating treatment strategies for acute ankle sprain and CAI. A secondary aim was to identify the current gaps in the literature for researchers, and identify any conflicting evidence between reviews.
Methodology
Protocol
The study protocol was developed using the framework described by Smith et al,9 which relates to the methodology of conducting a systematic review of systematic reviews of healthcare interventions. The protocol for the review was not pre-registered prior to its completion.
In January 2016, we undertook a computerised literature search of the following databases from inception: PubMed, PEDro, Scopus, Web of science, EBSCO and the Cochrane library.10 The database search was further supplemented with a manual search of the reference lists in each review. These processes retrieved a set of systematic reviews closely related to the treatment of ankle sprain injuries and CAI.
The empirical search strategy was developed in accordance with the recommendations outlined by Montori et al.11 The search strategy was constructed for MEDLINE and completed in a stepwise manner using the Boolean operators (table 1).
Search strategy
The search strategy was adapted for each database on the basis of previously published recommendations.12 No restrictions (including language) were applied in any of the databases when the search was completed. One investigator reviewed all the titles produced by the database searches, and retrieved suitable abstracts. After screening by abstract, full text articles were obtained for review (figure 2).
Inclusion/exclusion criteria
Our inclusion criteria were as follows: (1) the study must be a systematic review, which was defined as a research study that collects and evaluates multiple studies, and that limits inclusion bias of authors by using a clearly defined search strategy; (2) it must evaluate the efficacy of an intervention for the treatment and/or prevention of acute ankle sprain and/or CAI; (3) the efficacy of the intervention must be measured by means of an experimentally quantifiable outcome (detailed later). Patients with CAI were defined by having a history of at least one ankle sprain, a history of the previously injured ankle joint ‘giving way’ and/or recurrent sprain and/or ‘feelings of instability’.8 No restrictions were applied with regard to the intervention type or sample population of the studies included in the review papers.
Data extraction
A data extraction form was devised by all the authors. Data extraction was performed by one author. A random sample of studies were selected and doublechecked by a second author, to ensure quality. Data extraction included information related to both the review itself (including study details (author, year of publication and title), the injury type(s), outcome(s), intervention type(s) and main findings), and the individual studies included in the reviews (including study details (author, year of publication and title), design (randomised controlled trial (RCT)/non-RCT), sample population (% males vs females), experimental group N, control group N, injury type(s), intervention type(s), comparison type (s), protocol, outcome(s), findings (number of injuries in the control/experimental groups), conclusions). For studies in which an exercise therapy intervention was administered, the total ‘dose’ of the intervention (in minutes) was calculated and extracted.
Reviews were divided as to whether they concerned the treatment of acute ankle sprain or CAI (injury type). Owing to the potential overlap of treatment goals, any review that evaluated the efficacy of a prevention strategy for a new or recurrent ankle sprain with sufficient follow-ups (≥12 months) was also grouped into the ‘CAI treatment’ division, as recurrent ankle sprain is considered to be at the centre of the CAI paradigm.8 ,13 No restrictions were placed on the severity or type of ankle sprain sustained (lateral/medial/syndesmotic).
Intervention types were divided into surgical and non-surgical. Non-surgical interventions were further subclassified into physiotherapeutic (including exercise and manual therapies), external support (including taping, bracing and orthotics), electrophysical (including cryotherapy and any type of electrotherapies), pharmacological (including medications) and complementary (acupuncture; aromatherapy and herbal medicines) agents. These interventions were chosen following a thorough review of the literature and on the basis of the classification system used by Bleakley et al.14
The outcomes of interest were delineated into primary and secondary types. The primary outcomes were (re-) injury incidence/prevalence and/or self-reported function/disability based on a validated questionnaire for ankle joint function.13 The secondary outcomes included pain, strength, range of motion (ROM), proprioception and muscle activity in the region of ankle joint, in addition to performance measures (which included biomechanical analyses of static/dynamic postural control, gait or jumping/landing tasks). A schematic depicting the aforementioned classification system is depicted in figure 1.
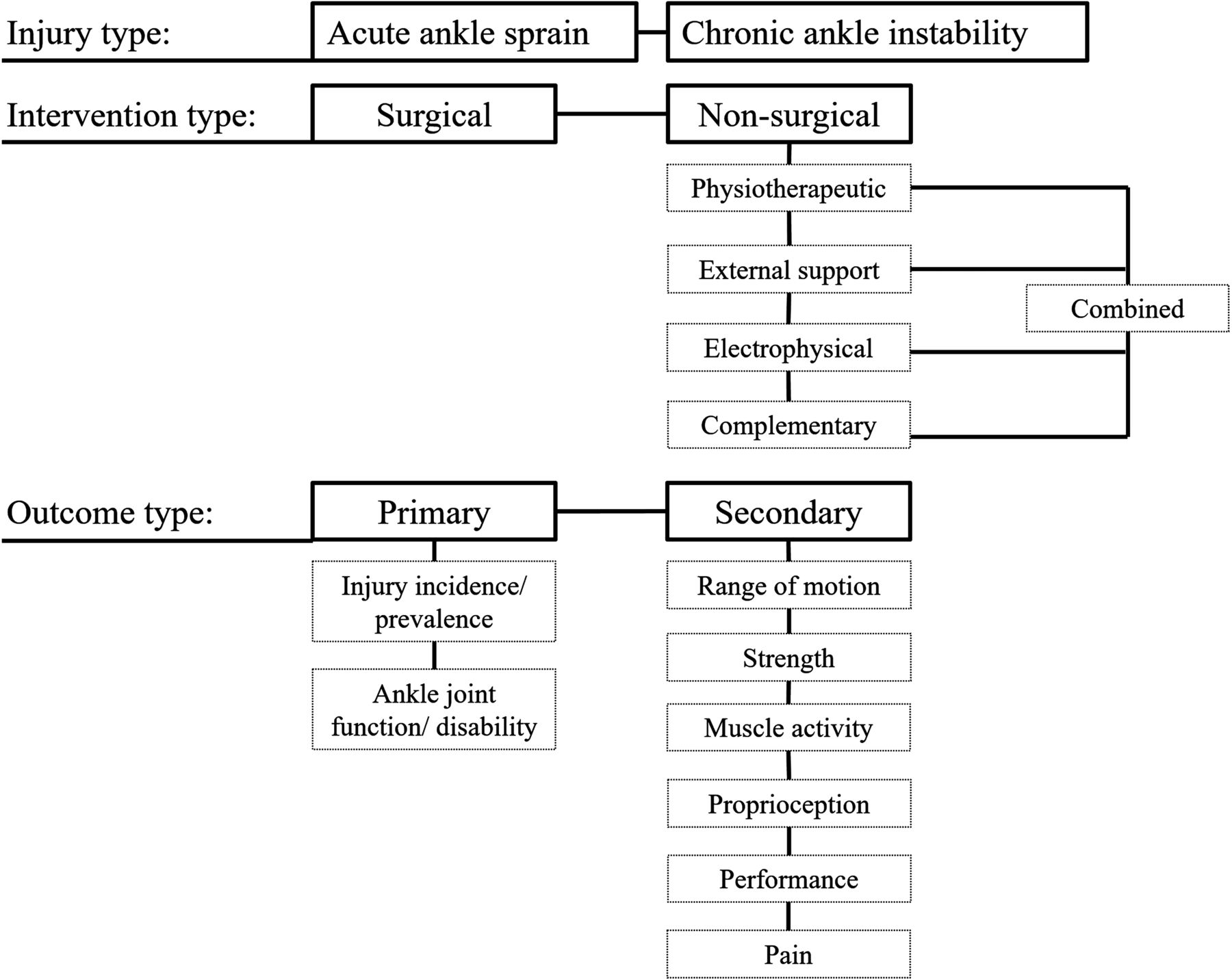
Schematic depicting the injury, intervention and outcome types by which the studies were stratified.
Risk of bias assessment
The quality of the systematic reviews was independently assessed by two authors (CD and SH) using the AMSTAR tool.15 Any disagreement between authors was resolved by group consensus. Where reviews provided an overall quality assessment of the included studies (items number 7/8 of the AMSTAR tool), those tools were extracted as potentially valuable research resources.
Analysis
The main conclusions from each systematic review concerning injury and intervention type were extracted. The reviews were categorised as ‘high’ or ‘low’ quality based on an arbitrary score of 7/11 on the AMSTAR quality rating. This ‘high- quality’ threshold was subsequently used to conduct a best evidence synthesis of the reviews. The outcomes, intervention type, main results and conclusions relating to our predefined primary and secondary outcomes (defined in data extraction) from the high-quality reviews (ie, rating ≥7) were compiled in tabular format, and stratified according to intervention type. This best evidence synthesis was conducted in order to provide a reference point for the interventions with the strongest evidence supporting or opposing their use.
Additionally, the individual papers included in each review were identified to determine; if they reported on any of the primary or secondary outcomes. The reference for each individual paper was extracted in such situations. In situations where there were contradictory conclusions from reviews then the individual quality rating of each review was presented (to contextualise a given conclusion to the overall quality of the review that made it); if the conclusions between different reviews were in agreement, the quality range (lowest and highest) of the reviews in question was presented.
Exploratory meta-analyses of the individual studies were performed for the primary outcome of (re-) injury incidence where possible. Only RCTs were included in pooling. Data (experimental group N and injuries after follow-up, control group N and injuries after follow-up; total dose of exercise (where appropriate)) were entered into the Cochrane Collaboration Review Manager (V.4.2) software program. Study effect estimates were calculated using ORs with 95% CIs. Studies were weighted by sample size. Data were assessed for heterogeneity based on the Q test in conjunction with the I2 statistic. The significance for χ2 was set at p<0.1. I² values >50% were considered to represent substantial heterogeneity.16 In cases where substantial heterogeneity was present, a random-effects model was used. Accordingly, OR values were used to enable several forest plots.
Results
Search results
The initial search strategy produced 2506 articles. A PRISMA diagram of the search strategy is available in figure 2. A total of 46 systematic reviews met the inclusion criteria.14 ,17–61 The quality of the included reviews is displayed in table 2.
Quality of the included reviews as rated on the AMSTAR scale

PRISMA flow diagram depicting the search protocol with stepwise article inclusion/exclusion. CAI, chronic ankle instability.
Forty of the reviews performed some kind of quality assessment of their included studies (see online supplementary table S2).
Supplemental material
Following the removal of duplicated papers, these reviews collectively included 309 individual reports. Additional information extracted from these studies segregated by injury and intervention is available in the online supplementary information for this article; due to the large volume of extracted information, only information relating to the primary outcomes (injury (re-)incidence/function) has been presented in the main text; all information related to the individual studies included in the reviews/the secondary outcomes is available in the supplemental documents. Please refer to the online supplementary table S1 for the results of the individual studies with respect to the primary and secondary outcomes.
There was a significant amount of overlap between the reviews regarding the injury type of interest, with 15 reviews being classified as investigating treatment strategies for both acute ankle sprain and CAI.14 ,17 ,19 ,24 ,28 ,32 ,34 ,37 ,41 ,43 ,45 ,50 ,52 ,53 ,60 Twenty reviews investigated treatment strategies for acute ankle sprain specifically.18 ,21–23 ,26 ,27 ,29–31 ,39 ,40 ,44 ,46–49 ,54 ,55 ,58 ,61 Nine reviews investigated treatment strategies for CAI specifically.20 ,33 ,35 ,36 ,42 ,51 ,56 ,57 ,59 Two reviews investigated treatment strategies for syndesmotic ankle sprain; however, these only included case studies and did not report on either of our primary or secondary outcomes.25 ,38 Eight of the reviews evaluated surgical interventions for the treatment of acute ankle sprain20 ,25 ,29 ,31 ,38–40 ,51 with 45 evaluating some kind of non-surgical intervention.14 ,17–61 The results and conclusions from the reviews ranking as ‘high’ quality have been synthesised in a best evidence synthesis table (table 3), stratified by the intervention type.
Results of the best evidence synthesis from the reviews deemed as ‘high’ (≥7 on the AMSTAR tool) quality. Only outcomes, results and conclusions relating to our predefined primary and secondary outcomes are displayed
Acute ankle sprain
Surgical interventions
Six reviews20 ,29 ,31 ,39 ,40 ,51 (quality range=5–10) compared surgical to non-surgical interventions for the treatment of acute ankle sprain. These reviews contained 82 individual (non-duplicate) papers. Of these 82, 33 (32 RCTs, 1 non-RCTs; N=4080; 65% male, 35% female) evaluated a surgical intervention specifically.62–94
None of these reviews reported on the primary outcome of recurrence. Function was determined by the time taken to return to activity/work.20 ,29 ,31 ,39 ,40 ,51 Of the six reviews, one (quality=6/11) advocated conservative management (including physiotherapeutic and external support interventions) over surgery,39 and two (quality=7/11;40 quality=5/1131) identified that surgery had better outcomes when compared with conservative management in the treatment of acute ankle sprain.31 ,40 One review (quality=9) found that there was insufficient evidence to determine the relative effectiveness of either surgical or conservative management in the treatment of an acute ankle sprain.29
Despite its projected benefits, several of the reviews identified the propensity for a surgical intervention to have a higher risk of complication (which included issues such as wound healing, infection, dystrophy, iatrogenic nerve damage leading to sensory deficit and paraesthesia) compared with a conservative intervention.20 ,29 ,31 ,39 ,40 A surgical intervention was also associated with greater financial cost.29 ,40
Non-surgical interventions
Physiotherapeutic
Eighteen systematic reviews evaluated a physiotherapeutic intervention for the treatment of acute ankle sprain14 ,17 ,19 ,23 ,29 ,31 ,32 ,39 ,41 ,44 ,45 ,50 ,52 ,53 ,58 ,60 ,61 ,95 (quality range=2–10), which themselves included 118 individual reports were included on removal of papers duplicated between each review. The two main kinds of physiotherapeutic intervention evaluated were exercise therapy and manual therapy.
Exercise therapy
Of the 18 separate systematic reviews, 1514 ,17 ,23 ,29 ,31 ,39 ,41 ,44 ,45 ,50 ,52 ,53 ,58 ,60 ,61 (quality range=2–10) evaluated the effectiveness of exercise therapy for the treatment of acute ankle sprain. Included in these reviews were 41 individual papers (33 RCTs, 8 non-RCTs; N=4680; 68% male, 32% female) where exercise therapy was the primary intervention for the treatment of acute ankle sprain.82 ,96–135
The reviews were unanimous in their consensus that exercise therapy improves self-reported function following acute ankle sprain.3 ,14 ,17 ,23 ,41 ,44 ,52 ,53 ,60 ,61 Three of the reviews reported on the primary outcome of recurrence in a sample of individuals with acute ankle sprain.14 ,39 ,60 All three confirmed the effectiveness of exercise therapy for the prevention of recurrence following an acute ankle sprain.4 ,14 ,39 ,60
Manual therapy
Of the 18 separate systematic reviews that evaluated a physiotherapeutic intervention, 514 ,19 ,32 ,45 ,50 (quality range 5–10) evaluated the effectiveness of manual therapy for the treatment of acute ankle sprain. Included in these reviews were 12136–147 individual papers (all RCTs, N=687) in which some form of manual therapy technique was used in the treatment of acute ankle sprain.5
It is unclear whether manual therapy was beneficial for the primary outcomes of self-reported function or injury recurrence.6 ,7 ,14 ,19 ,32 ,45 ,50
Electrophysical agents
Seven systematic reviews evaluated an electrophysical intervention of some kind for the treatment of acute ankle sprain14 ,18 ,45 ,49 ,52 ,53 ,95 (quality=6.7).2 Fifty papers (on removal of duplicates) were included in these reviews. Of these 50 papers, 21 (all RCTs, N=1459; 59% male, 41% female) evaluated the effectiveness of an electrophysical agent in the treatment of acute ankle sprain.8 ,120 ,124 ,148–166
Applications of ice and compression or the use of elevation do not seem to be effective for improving the primary outcomes of self-reported function or recurrence following acute ankle joint sprain compared with no treatment.18 ,95 Three reviews concluded that treatment success was achieved on the basis of an exercise therapy intervention that was often combined with a rest/ice/compression/elevation (RICE) protocol.52 ,53 ,95
None of the reviews determined any beneficial effect of ultrasound therapy in the treatment of acute ankle sprain.14 ,49 However, there are very few trials evaluating the effectiveness of ultrasound therapy for acute ankle sprains,49 and fewer still have considered the range of intervention parameters available.14 ,49 Similarly, the evidence for the efficacy of laser, electrical stimulation and hyperbaric oxygen therapies is limited due to a lack of related research.14 ,45
External support
Six systematic reviews evaluated an external support of some kind for the treatment of acute ankle sprain26 ,28 ,39 ,44 ,53 ,61 (quality range 3–10). These reviews included 46 individual papers. Twenty-four of these (23 RCTs, 1 non-RCT; N=2141, 66% male, 34% female) evaluated some kind of external support (which included taping, bracing and orthoses9) in the treatment of acute ankle sprain.103 ,105 ,116 ,126 ,135 ,167–185
The reviews were unanimous in their consensus that braces and taping are effective in the treatment of acute ankle sprains for the primary outcomes of self-reported function and recurrence.10 ,11 ,26 ,28 ,39 ,44 ,53 ,61
Complementary
Three systematic reviews evaluated some kind of complementary medicine for the treatment of acute ankle sprain14 ,30 ,37 (quality range 5–10). These three reviews included 60 individual papers. There were two papers duplicated between these reviews, leaving 58 individual reports. Of these 58, 35 (all RCTs; N=2358, 67% male, 33% female) evaluated some kind of complementary medicine in the treatment of acute ankle sprain.186–220 Acupuncture was the primary focus of the reviews however.14 ,30 ,37
Two of the reviews (quality=5/11;14 10/1130) reported that there were insufficient data to determine the relative effectiveness of complementary medicine in the treatment of acute ankle sprain for self-reported function or injury recurrence.12
The final review (quality=9/11) concluded that acupuncture was likely to have a therapeutic effect in improving acute symptoms, but acknowledged that the results were likely to be overestimated due to the low quality of the included studies.37
On this basis, the evidence for the efficacy of complementary therapies in the treatment of acute ankle sprain for the primary outcomes of injury recurrence/self-reported function is inconclusive.
Pharmacological
Three systematic reviews evaluated some kind of pharmacological intervention for the treatment of acute ankle sprain14 ,30 ,44 (quality range 3–10). These reviews included 47 papers (all RCTs; N=6395, 62% male, 38% female). There were no duplicated papers between these reviews. Thirteen papers (N=2423, 47% male, 53% female) evaluated any pharmacological agent (which typically included non-steroidal anti-inflammatory drugs) in the treatment of acute ankle sprain as the primary intervention.13 ,136 ,186 ,187 ,196 ,199 ,220–226
Owing to the short follow-up periods in the individual studies, no conclusions could be made for the primary outcomes of self-reported function or injury recurrence.
Chronic ankle instability
None of the included reviews evaluated the efficacy of electrophysical agents, pharmacological interventions or complementary medicine for the treatment of CAI or recurrent ankle sprains.
Surgical interventions: CAI
Two reviews20 ,51 (quality range 6–10) evaluated the efficacy of surgery for the specified treatment of CAI or recurrent ankle sprains.14 Included in these reviews were 24 individual papers, 8 of which evaluated a surgical intervention for the treatment of CAI or chronic recurrent ankle sprain (all RCTs; N=533; 64% male, 36% female).62–64 ,71 ,72 ,94 ,227 ,228
None of the reviews specifically investigated whether a surgical intervention was superior to conservative management for CAI. In the majority of individual studies, a surgical intervention was often implemented provided conservative management had failed.62–64 ,94 ,227 ,228 Furthermore, none of the individual reports had a non-surgical control group,51 and none of the studies reported on the primary outcome of reinjury incidence.15 ,62–64 ,71 ,72 ,94 ,227 ,228
Non-surgical interventions: CAI
Twenty-three reviews evaluated the efficacy of a physiotherapeutic intervention (which included exercise and manual therapies) in the treatment of CAI or recurrent ankle sprain17 ,19 ,20 ,23 ,32–36 ,41–43 ,45 ,46 ,50 ,51 ,54–57 ,59–61 (quality range 1–10). Following the removal of duplicates, these reviews included 122 individual papers (83 RCTs, 39 non-RCTs; N=26349, 82% male, 18% female).
Exercise therapy
Twenty-two of the included reviews evaluated exercise therapy for treating CAI or recurrent ankle sprain17 ,19 ,20 ,23 ,33–36 ,41–43 ,45 ,46 ,50 ,51 ,54–57 ,59–61 (quality range 1–10). Included in these reviews were 114 individual reports, 61 of these papers evaluated the efficacy of exercise therapy for the treatment of CAI or recurrent ankle sprain specifically (42 RCTs, 19 non-RCTs; N=13963; 70% male, 30% female).65 ,96–99 ,101–104 ,106 ,107 ,110–113 ,118 ,119 ,121–123 ,128–135 ,229–261
Exercise therapy is generally considered effective in the treatment of CAI for the outcomes of self-reported function20 ,23 ,41 ,45 ,51 ,57 ,60 and reinjury incidence.16–20 ,33–36 ,42 ,43 ,46 ,50 ,51 ,54 ,55 ,60
Manual therapy
Five reviews19 ,32 ,45 ,50 ,51 (quality range 6–10) evaluated the effect of ankle joint mobilisation in CAI populations. Of the 122 individual papers included in these reviews, 12 (all RCTs, N=340; insufficient data to calculate male:female ratio) evaluated some kind of manual therapy in the treatment of ankle sprain.137–147 ,262
Regarding the primary outcomes of self-reported function or injury recurrence, five of the individual papers included samples with CAI or recurrent ankle sprains139 ,142 ,144 ,146 ,262 and one reported on the primary outcome of self-reported function with a follow-up period that was not immediately post-treatment.21 ,139
All the reviews identified that manual mobilisation is likely to have a (initial) positive effect on ankle dorsiflexion ROM.19 ,32 ,45 ,50 ,51
External support
Nine systematic reviews evaluated the efficacy of an external support intervention for the treatment of CAI21 ,22 ,24 ,34 ,46 ,47 ,54 ,55 ,61 (quality range 4–10). These reviews included 115 papers. Of these 115, 63 individual reports were included after removal of papers duplicated between each review. Of the 63 individual reports, 39 (15 RCTs, 24 non-RCTs; N=8734; 90% male, 10% female) evaluated some kind of external support for the treatment of CAI.108 ,173 ,247–262 The primary outcome in all of the reviews was reinjury incidence.
There was unanimous consensus among the reviews that bracing is effective at preventing a recurrence of an ankle sprain.21 ,22 ,24 ,34 ,46 ,47 ,54 ,55 ,61 With regard to taping, two reviews (quality=5/11;46 4/1122) concluded that its efficacy could not be supported (and that bracing was superior) whereas three reviews (quality=5/11;55 4/11;54 9/1121) advocated its value in the prevention of ankle sprain recurrence. It remains unclear whether bracing or taping are effective interventions for the primary prevention of an ankle sprain.21 ,24 ,54
The reviews identified that the evidence for modified footwear was inconclusive in the prevention of ankle sprain or its recurrence.23 ,46 ,47 ,54
There was a lack of evidence for the value of orthotics in the treatment of CAI or the prevention of ankle sprain recurrence.22 ,24
Meta-analysis
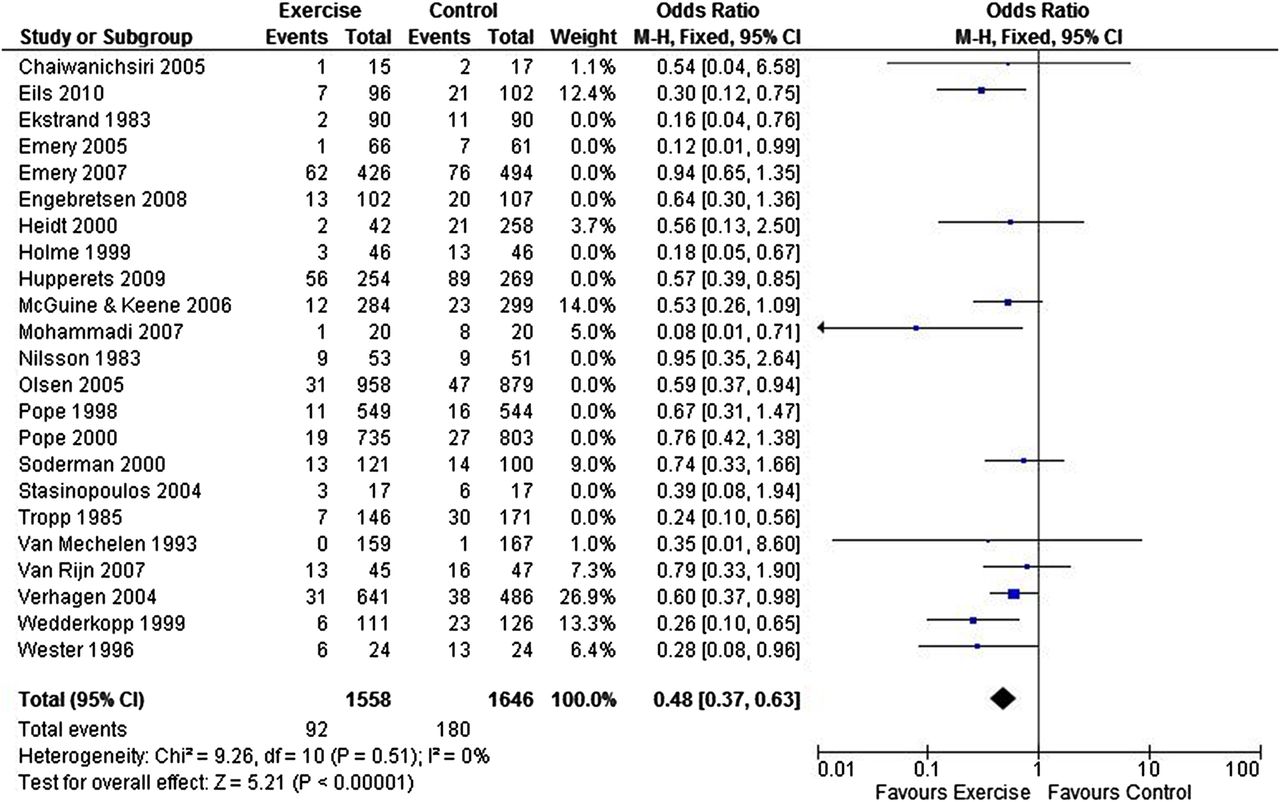
Exercise interventions significantly decreased the risk of sustaining a recurrent ankle sprain (figure 3; OR=0.59, 95% CI 0.51 to 0.68). An exploratory sensitivity analysis by treatment dose (high dose vs low dose using a median split of 900 min) was performed. Removal of interventions with a lower dose of total exercise (<900 min) improved the odds of the exercise intervention for injury risk (figure 4; OR=0.48, 95% CI 0.37 to 0.63). A summary of the exercise therapy interventions (with overall study quality) presented in the individual papers is presented in online supplementary table S3.
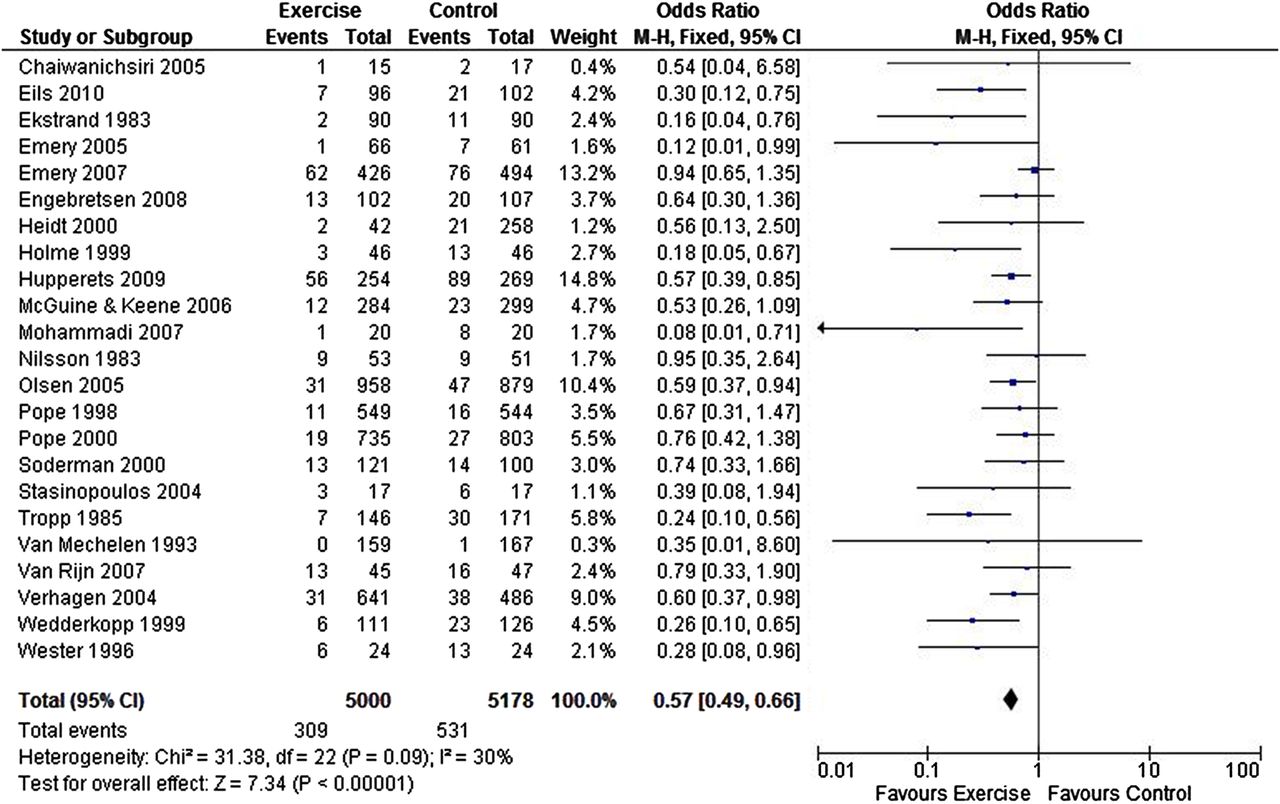
Forest plot depicting the results of the meta-analysis for exercise interventions in the treatment of recurrent ankle sprain injury.
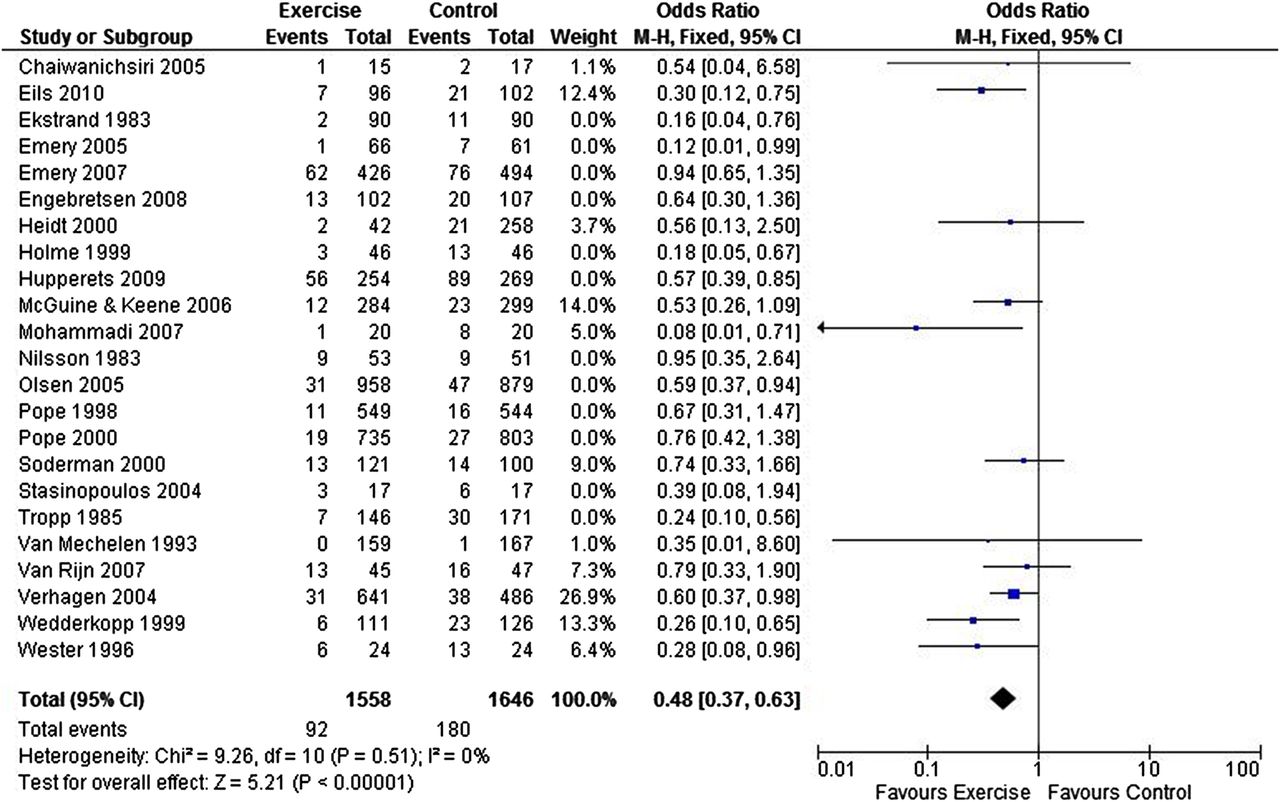
Forest plot depicting the results of the meta-analysis for high-dose exercise interventions only in the treatment of recurrent ankle sprain injury.
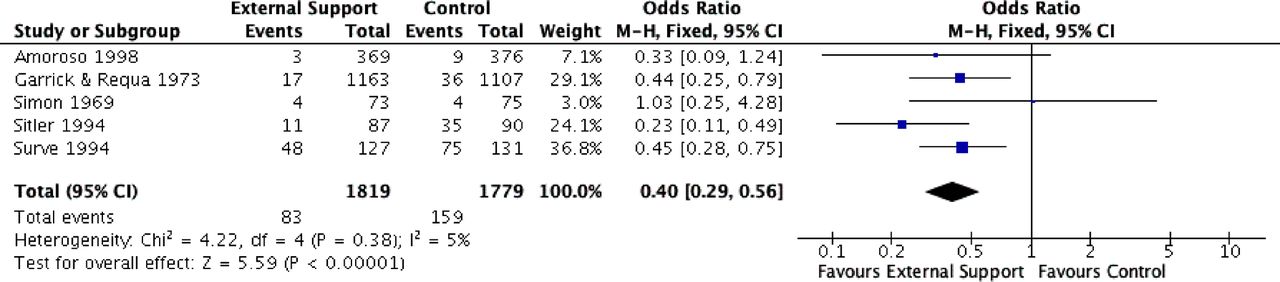
External support interventions were also associated with a significantly decreased risk of sustaining a recurrent ankle sprain (figure 5; OR=0.38, 95% CI 0.30 to 0.47).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot depicting the results of the meta-analysis for bracing interventions in the treatment of recurrent ankle sprain injury.
Discussion
This systematic review of treatment strategies for acute ankle sprain and CAI found 46 reviews which included 309 individual studies. As the conclusions of each review have been presented, the following topics in the treatment of acute ankle sprain/CAI will be clarified and discussed: surgical interventions; conservative interventions; treatment of specific types of ankle sprain.
Surgical interventions
Treatment strategies in the current review were divided into surgical and non-surgical types. The surgical literature is sparse however, and never were the long-term effects of a surgical intervention on the primary outcome of recurrence investigated. The general consensus of the reviews that investigated a surgical intervention was that a trial of conservative treatment should always be attempted before surgery is undertaken, that surgery should be considered only in patients with persistent symptoms, and that it should be considered on an individual basis.29 ,39 ,40
Conservative interventions
Meta-analysis
Owing to a significant heterogeneity of outcomes, samples, interventions and follow-up periods, meta-analyses were only undertaken to evaluate the effect of exercise and external support interventions on reinjury in individuals with a history (acute or chronic) of ankle sprain. This analysis elucidated that an exercise intervention can significantly reduce the odds of ankle sprain recurrence, and that this effectiveness is improved if the exercise therapy is given in high (>900 min of exercise therapy training) doses. The other meta-analysis conducted as part of this investigation advocated the use of an external support in reducing the odds of ankle sprain recurrence. The review papers equated the efficacy of taping with bracing54 ,55 (with a similar reinjury risk reduction of 50%,55 while also reducing the severity of the incurred sprain25 ,54).
Exercise therapy
A number of limitations in the available research were acknowledged in the reviews and as such, the findings of the meta-analysis for exercise therapy should be interpreted with caution. First, many of the authors stated that the studies included in their reviews were very heterogeneous.17 ,20 ,36 ,51 ,60 ,61 With regard to the statistical pooling performed as part of the current investigation, reflection of the exercise programmes implemented in the individual papers highlights this heterogeneity (see online supplementary table S2). Additionally, information regarding the intervention parameters was not adequately described in most studies. Furthermore, several reviews endorsed the completion of additional high-quality research to identify the specific parameters (such as the dose, intensity, type) of exercise therapy required to improve long-term outcomes.35 ,41 ,56 ,57 ,60 It is also currently unknown as to whether exercise therapies reduce the severity of an ankle reinjury, or increase the number of exposures before an ankle injury occurs.34 Finally, there is a lack of evidence which links improvements in the primary outcomes with improvements in secondary outcomes111 (which could elucidate the mechanistic underpinnings of treatment efficacy).
External supports
Generally, the conclusions of the systematic reviews for an external support that included a taping or bracing intervention identified that their benefit could be enhanced with an appropriately designed exercise therapy programme and that the efficacy of these interventions may be ‘additive’ in the secondary prevention of ankle sprains.55 Braces were recommended for all athletes with a previous history of ankle sprain, particularly when engaging in high-risk activities such as indoor/court and field sports.22 ,24 It was recommended that a brace be worn for a minimum of 6 months after an acute ankle sprain to prevent recurrence,46 ,47 and that the benefit of wearing a brace lasts for up to 1 year following the most recent ankle sprain.54 Next to the recognised preventive effect, the use of external support was considered to result in less severe ankle sprains.54 With regard to the type of external support recommended, Kerkhoffs et al28 and Seah and Mani-Babu44 both concluded that lace up ankle supports were superior to semirigid ankle supports.
Manual therapy
Studies on the effect of the physiotherapeutic intervention of manual therapy were limited by short follow-up time frames which impeded extrapolation of the long-term benefits of these techniques for either of the primary outcomes.19 ,32 ,45 ,50 ,51
Electrophysical agents
No review investigated the efficacy of electrophysical agents in the treatment of CAI. Electrophysical agents were not considered effective treatments for acute ankle sprain. However, the standard practice of applying ice and compression (or the use of elevation) is generally administered concurrently with an exercise therapy intervention.52 ,53 ,95 While it is unknown if a RICE protocol augments the effect of exercise,18 given the strong empirical evidence base and the popularity of cryotherapy treatment (particularly for the secondary outcome of pain), it may be difficult to randomise a participant to a ‘no ice’ group.18 In conjunction with this point, a number of reviews recognised the paucity of high-quality studies evaluating an electrophysical agent in the treatment of acute ankle sprain.14 ,18 ,53 ,95
Complementary medicine
Similarly, complementary medicine has not been investigated in the treatment of CAI, and is not considered to be effective in the treatment of acute ankle sprain. Both the relevant reviews identified that there seemed to be a short-term benefit of complementary medicine for the secondary outcomes of pain and swelling, but cited that it remains unclear as to whether this is clinically meaningful in the long-term for injury recurrence and self-reported function.14 ,30
Ankle sprain type
Finally, only two of the reviews evaluated treatment strategies in the management of syndesmotic ankle sprain; the individual papers included in these reviews were all case studies and as such, no meaningful results could be drawn from them. No reviews were identified which sought to investigate treatment strategies for medial ankle sprain. The remaining reviews either did not present a specific definition of the type of ankle sprain (lateral/medial/syndesmotic), or focused on the most prevalent subtype of this injury: a lateral ankle sprain.1 Future research is required to identify the optimal management strategies for medial and syndesmotic ankle sprains.
Limitations with this review
This review itself is not without limitations. First, due to the inherent nature of this type of study design, the latest literature is unlikely to be included in even the most recently published systematic reviews and is therefore omitted from this article. Additionally, data extraction was conducted by only one author; while all the authors were involved in devising the data extraction form and two performed the quality review, our protocol could have been improved if two authors had independently extracted the data. A sample of the studies was randomly selected to be double checked by a second author, to ensure quality. However, due to the volume of data and time-intensive nature of this, it was unfeasible for a second author to double extract the data.
Conclusion
This review summarises the evidence base for a number of interventions designed to treat and prevent acute ankle sprain and CAI. The best evidence synthesis of high-quality reviews indicates there is strong evidence for exercise therapy and bracing in preventing recurrence of an ankle sprain. The efficacy of surgery and acupuncture are controversial in the treatment of acute ankle sprains. There is insufficient evidence examining the effectiveness of ultrasound in the treatment of acute ankle sprains.
What are the findings?
A large number of systematic reviews detail treatment strategies for ankle sprain.
This makes appraisal of the literature difficult for clinicians.
The optimal treatment strategy for acute/recurrent ankle sprain is unclear.
However the best evidence synthesis indicates there is strong evidence for exercise therapy and bracing in preventing ankle sprain recurrence.
How might it impact on clinical practice in the future?
Exercise therapy and taping/bracing are effective in the management of acute/recurrent ankle sprain.
There is a lack of evidence for the effectiveness of ultrasound therapy, acupuncture and manual therapy in the treatment of recurrent ankle sprain.
Surgery for acute/recurrent ankle sprain should only be considered on an individual basis.
Acknowledgments
Collaborating associations/institutes: The Insight Centre for Data Analytics, School of Public Health, Physiotherapy and Sports Science and the Institute for Sport and Health (University College Dublin), and the Sport and Exercise Sciences Research Institute (Ulster Sports Academy, University of Ulster).
References
Footnotes
Twitter Follow Sinead Holden at @Sinead_Holden, Cailbhe Doherty @DohertyCailbhe, Chris Bleakley @ChrisMBleakley, Eamonn Delahunt @EamonnDelahunt
Contributors CD and SH had equal contribution and act as guarantors. They conceived the study and acquired the data. CD, SH and CB analysed the data. All authors drafted the manuscript. All authors critically revised the manuscript pre- and post-peer review.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.