Article Text

Abstract
Objective Given the high exposure to occupational standing in specific occupations, and recent initiatives to encourage intermittent standing among white-collar workers, a better understanding of the potential health consequences of occupational standing is required. We aimed to review and quantify the epidemiological evidence on associations of occupational standing with musculoskeletal symptoms.
Design A systematic review was performed. Data from included articles were extracted and described, and meta-analyses conducted when data were sufficiently homogeneous.
Data sources Electronic databases were systematically searched.
Eligibility criteria Peer-reviewed articles on occupational standing and musculoskeletal symptoms from epidemiological studies were identified.
Results Of the 11 750 articles screened, 50 articles reporting 49 studies were included (45 cross-sectional and 5 longitudinal; n=88 158 participants) describing the associations of occupational standing with musculoskeletal symptoms, including low-back (39 articles), lower extremity (14 articles) and upper extremity (18 articles) symptoms. In the meta-analysis, ‘substantial’ (>4 hours/workday) occupational standing was associated with the occurrence of low-back symptoms (pooled OR (95% CI) 1.31 (1.10 to 1.56)). Evidence on lower and upper extremity symptoms was too heterogeneous for meta-analyses. The majority of included studies reported statistically significant detrimental associations of occupational standing with lower extremity, but not with upper extremity symptoms.
Conclusions The evidence suggests that substantial occupational standing is associated with the occurrence of low-back and (inconclusively) lower extremity symptoms, but there may not be such an association with upper extremity symptoms. However, these conclusions are tentative as only limited evidence was found from high-quality, longitudinal studies with fully adjusted models using objective measures of standing.
- Review
- Meta-analysis
- Lower back
- Work
- Lower limb
Statistics from Altmetric.com
Introduction
Exposure to extended periods of occupational standing is traditionally common among specific occupational groups, such as in the retail, food, healthcare, education and manufacturing industries. For example, in a population of Australian workers, 62% reported working in a job that usually involved standing,1 a finding consistent with that observed in a study conducted with a Canadian working population.2 In a study with objectively measured standing (using thigh-worn and hip-worn accelerometers), it was shown that Danish blue-collar workers stood on average 2.2 (SD 1.3) hours per workday with subgroups standing for up to 3.7 (0.7) hours per workday.3
A recent and growing body of evidence suggests that excessive sitting is associated with several adverse health outcomes including poor cardiometabolic health and premature mortality.4–6 Consequently, there is a growing interest in workplace initiatives to reduce the amount of sitting time for sedentary workers,7 with expert recommendations advising workers to replace some sitting periods with standing and light activity at work,8 specifically by advocating regular postural changes (ie, shifting between sitting, standing and moving). Replacing sitting with alternatives such as standing has been shown to be feasible,8 ,9 and is rapidly being implemented in many workplaces, such as through the introduction of sit/stand office workstations.10 However, some concerns have been expressed that alternatives to sitting, such as standing, may expose workers to new hazards and/or other health consequences.11
In light of shifting working styles, a sound understanding of the health consequences of occupational standing is urgently needed to inform healthy work practice for blue-collar and white-collar workers. Adverse health outcomes of standing have been reported before,12 with standing being associated with venous disorders of the lower extremities,13 ,14 perinatal health complications such as preterm delivery and pre-eclampsia,15 and musculoskeletal symptoms such as low-back and lower limb symptoms.16 ,17 However, previous reviews of the association of occupational standing with musculoskeletal symptoms (eg, self-reported pain, discomfort or symptoms in regions of the musculoskeletal system) have arrived at very different conclusions,18 ,19 and there has been criticism of their conclusions.20 ,21 The aims of this study were to systematically review the epidemiological evidence on the associations of occupational standing with non-specific musculoskeletal symptoms, and to quantify this association by means of meta-analyses.
Methods
Search strategy
To identify relevant publications, we performed systematic searches of the literature in the following bibliographic databases: Health & Safety Science Abstracts (Proquest); CINAHL (EBSCO); EBM Reviews—Cochrane Central Register of Controlled Trials (Ovid); EMBASE (Ovid); MEDLINE (Ovid); PsycInfo (Ovid). Searches were performed from database inception to 10 February 2015 with search terms including controlled key terms as well as free-text terms. Search terms expressing ‘standing’ were used in combination with search terms for ‘work-related’ (see online supplementary appendices 1–6). No specific terms for ‘health outcomes’ were used as this study is part of a larger review aimed at assessing the association of occupational standing with multiple health outcomes.
supplementary appendices
Two reviewers independently screened all potentially relevant titles and abstracts for eligibility. If necessary, full-text articles were checked for eligibility. Differences in judgement were resolved through a consensus procedure. Studies were included if they met the following criteria: the article was an original epidemiological study published in a peer-reviewed journal (ie, excluding reviews, editorials or letters, theses and conference proceedings); it was published in English; and it reported on the association between occupational standing and any health problem. Only articles that described a general adult working population were included (eg, studies selecting workers with chronic disorders and non-adult populations were excluded). Only studies quantifying the association of occupational standing with health outcomes were included (thereby excluding qualitative research). Studies in which occupational standing was not a main exposure variable of interest (eg, standing was only part of a certain condition/trial such as ‘lifting during standing’ or was part of a combined exposure such as ‘standing/walking’), or in which occupational standing was only used as a confounding variable, were excluded.
All eligible full-text articles were classified on exposure (work related vs non-work related), outcome (musculoskeletal or other outcomes) and study design (eg, laboratory study, cross-sectional study or longitudinal study). For the current study, only articles describing epidemiological cross-sectional (case–control or cross-sectional observational studies) or longitudinal observational studies on occupational standing and their association with musculoskeletal symptoms (ie, self-reported pain, discomfort and/or symptoms in any region of the musculoskeletal system) were included. Full-text versions of the selected articles were obtained for data extraction and quality assessment. In cases where full-text articles could not be found through online and/or offline databases, authors were contacted. Reference lists of selected articles were screened to identify additional potentially eligible articles.
Data extraction and quality assessment
Two reviewers independently assessed all selected articles for methodological quality and data extraction. In cases of disagreement, consensus was reached during a meeting. Methodological quality was evaluated using an adapted version of a published scoring system,22 based on 11 criteria for the reporting of study methods (description of recruitment, participants, allocation, measures, sample size) and results (description of variance, confounding, detail of results), with answer categories being ‘yes’, ‘partial’, ‘no’ and ‘not applicable’ (see online supplementary appendix 7). Summary scores (ranging from 0 to 1) were calculated with:
Studies with a summary score ≥0.75 were considered to be of high methodological quality.22
For data extraction, the following data from each included article were obtained: first author and year of publication, study name, study design, sample description (ie, number of participants, age, gender, occupation and country), confounders, exposure (assessment and operationalisation of occupational standing), outcome (assessment and operationalisation of musculoskeletal symptoms) and exposure–outcome estimates (eg, ORs, relative risks).
Data-analysis
All included studies were described according to their methodological quality and extracted data. Included articles were categorised into body areas regarding their outcomes; that is, low-back symptoms, lower extremity symptoms, upper extremity symptoms and symptoms in any body area.
In each of the four body areas, quantitative analyses of homogeneous studies (with sufficient overlap in definitions of exposure, outcome, study population and study design for which small differences in definition of exposure and outcome were accepted23) were performed if possible. To be able to combine information from different studies, occupational standing was treated as a dichotomous variable for which a cut-off value of 4 hours/workday was adopted (ie, durations of standing below this threshold were considered ‘not substantial’ while durations of standing above this threshold were considered ‘substantial’ standing). In the absence of any known ‘threshold’ for substantial standing, we selected this cut-off value based on the data provided in the identified studies with 4 hours/workday being the most often reported (with sensitivity analysis examining other thresholds). The cut-off is also consistent with the recent recommendations for those occupations which are predominately desk-based whereby the eventual progression to a total accumulation of up to 4 hours/workday is advocated to offset the health hazards associated with excessive sitting.8 Model parameters (ie, unadjusted ORs; or cross-tabulations of participants exposed to not substantial and substantial standing, with and without musculoskeletal symptoms) were retrieved from the original studies. If needed, exposure categories from studies reporting multiple occupational standing categories were collated. In instances where data provided in the published articles were insufficient, corresponding authors were contacted and asked for additional information.
Review Manager (RevMan) V.5.3 was used to conduct meta-analyses and generate forest plots, using a random-effects model due to the heterogeneity of the studies. We report on ORs with 95% CIs depicting each individual study as well as pooled exposure–outcome associations of substantial occupational standing and musculoskeletal symptoms, unadjusted for confounders. p Values <0.05 (two-sided) were considered statistically significant. Heterogeneity was assessed using I2 statistics and visual inspection of the forest plots were performed, while subgroup analyses were conducted using χ2 statistics. Funnel plots were generated to assess publication bias (through visual inspection).
Sensitivity analyses were conducted to test the robustness of pooled exposure associations. The sensitivity of the cut-off value for substantial occupational standing (4 hours/workday) was tested by comparing those studies for which we could estimate exposure–outcome associations with a 4 hours/workday cut-off value to those for which we could estimate exposure–outcome associations with a 2 hours/workday cut-off value (performing subgroup analysis). Owing to a lack of sufficient homogeneous data, we were not able to test for the effect of other cut-off values. In a second sensitivity analysis, we compared exposure–outcome associations unadjusted for confounders to exposure–outcome associations adjusted for confounders (eg, gender, age, other physical or mental work demands). We also tested for differences in exposure–outcome associations of studies reporting on generic samples of workers (ie, random samples of a general working population or samples of mixed occupational groups) compared with studies on samples of specific occupational groups (eg, only hospital staff, only construction workers). In a final sensitivity analysis, we tested for differences in exposure–outcome associations of studies with low compared with high methodological quality.
Results
Data description
The flow chart of the search and selection process is presented in figure 1. Our search strategy yielded a total of 15 857 search hits. After removing duplicates, 11 750 individual articles remained that were screened on their titles for inclusion. After excluding 10 951 records, a total of 799 abstracts were screened after which 356 abstracts did not meet the inclusion criteria. A total of 11 full-text articles could not be retrieved (even after contacting corresponding authors), providing a total of 432 full-text articles that were screened on eligibility, of which 218 met the criteria of describing outcomes of occupational standing. A total of 44 of these articles specifically addressed the association of occupational standing and musculoskeletal symptoms using an epidemiological study design. After screening the reference lists of these articles, six more articles were added, resulting in a final total of 50 articles (reporting 49 studies) included in the current review and used for methodological quality assessment and data extraction (table 1 for a summary of findings).17 ,24–72
Summary of findings from all identified evidence describing the number of studies (N) and number of participants (n) in each of the outcome (body area), study design, exposure assessment and study findings by categories
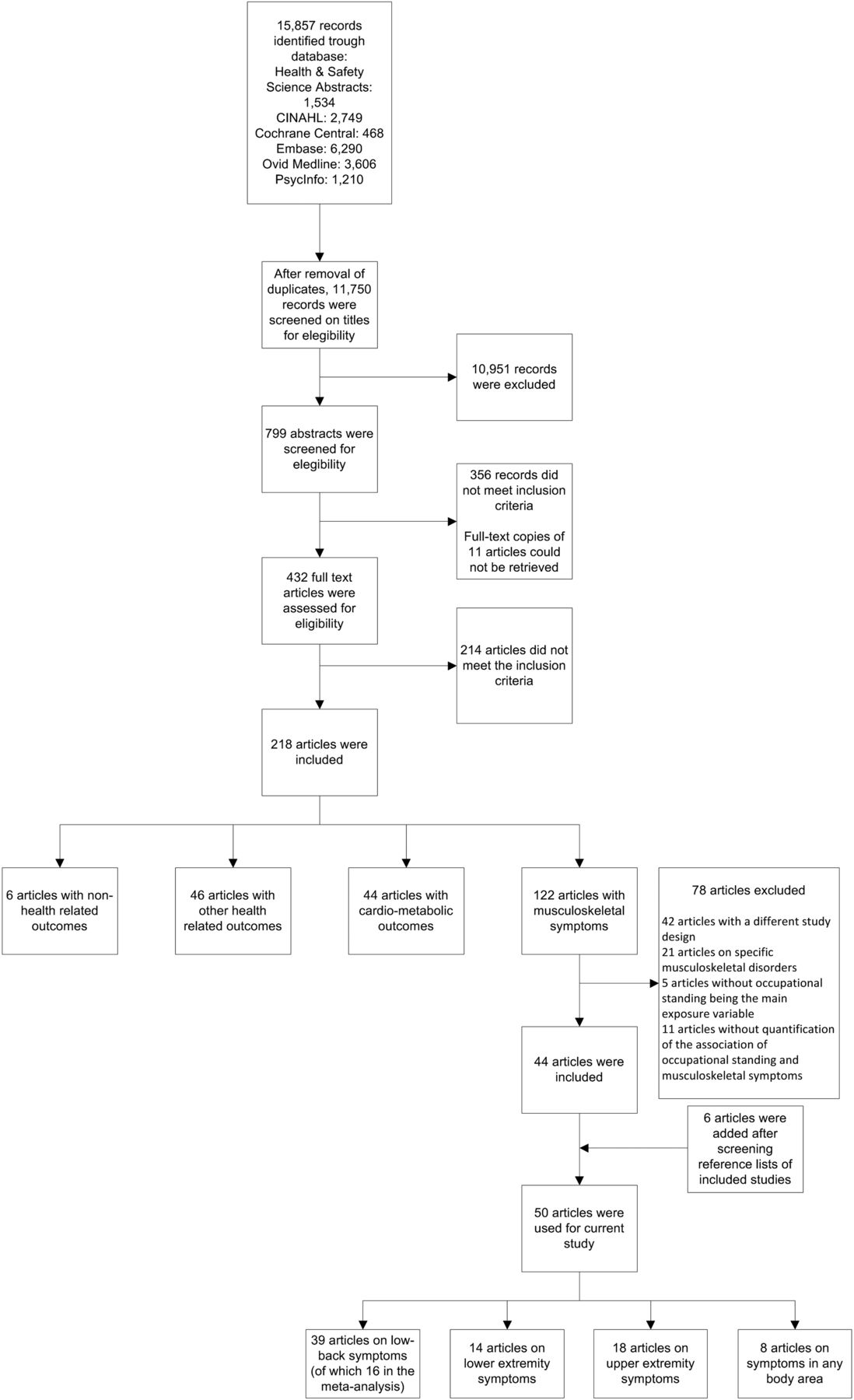
Flow chart, depicting the procedure of selecting articles.
The methodological quality of all included articles is shown in online supplementary appendix 8. The average methodological quality of the included articles was 0.79 (SD 0.16) out of 1, ranging from 0.23 to 1.00, with 32 articles describing a study considered to have high (≥0.75) methodological quality. Data extracted from the selected articles are presented in online supplementary appendix 9. Seven articles reported on a cross-sectional case–control study,24 ,33 ,35 ,36 ,48 ,49 ,56 38 a cross-sectional observational study,25–32 ,34 ,38–40 ,42–47 ,50–55 ,57–61 ,63–70 ,72 and 5 articles a longitudinal observational study.17 ,37 ,41 ,62 ,71 Forty-six articles reported occupational standing assessed by self-reports,17 ,24 ,26–35 ,37–50 ,52–59 ,61–72 two articles described occupational standing assessed by observations51 ,60 and two other articles described objectively measured (using accelerometers) occupational standing.25 ,36 A total of 46 articles reported on samples of workers recruited from a general (not exclusively worker) population and/or a work population,17 ,24–27 ,30–47 ,49–55 ,57–72 while 4 others reported on data from samples of workers that were recruited through a clinical setting.28 ,29 ,48 ,56 A total of 21 articles reported on random samples drawn from the general (working) population or samples of mixed occupational groups,17 ,28–30 ,33 ,36 ,37 ,41 ,47–49 ,51 ,52 ,54 ,56 ,59 ,62–65 ,70 and 29 articles reported about specific occupational groups, including healthcare workers,25–27 ,31 ,35 ,38–40 ,43–45 ,50 ,53 ,57 ,67 ,68 ,71 factory and assembly workers,32 ,34 ,60 ,61 teachers,58 ,72 farmers,55 ,69 and construction workers.42
Low-back symptoms
A total of 39 articles (n=82 229 participants in total) reported on the association of occupational standing with back symptoms, of which 33 focused on low-back symptoms,17 ,25 ,27–31 ,33 ,37–39 ,42–44 ,48–50 ,53 ,54 ,58–66 ,68–72 and 6 on back symptoms in general26 ,32 ,34 ,35 ,47 ,67 (all referred to as low-back symptoms from here). Sixteen articles (13 cross-sectional studies32 ,42 ,43 ,48–50 ,54 ,63–66 ,68 ,70 and 3 longitudinal studies,37 ,62 ,71 n=54 392 participants in total) provided sufficiently homogeneous information to conduct a meta-analysis, pooling exposure–outcome associations on substantial occupational standing and low-back symptoms. This resulted in a pooled OR (with 95% CI) of 1.31 (1.10 to 1.56), with I2=90% heterogeneity (figure 2; table 2). Associations found in studies with longitudinal study designs (1.17 (0.64 to 2.14)) were not statistically significant and the point estimate was slightly weaker compared with studies with cross-sectional study designs (1.32 (1.09 to 1.59)).
Summary of findings from meta-analyses describing the association of occupational standing and low-back symptoms

{kind=link}
{kind=link}
Forest plot of the unadjusted association of occupational standing (not-substantial standing vs substantial standing, adopting a 4 hours/workday cut-off value when possible) with low-back symptoms. Individual study, as well as pooled exposure outcome, associations are presented. Data from cross-sectional (upper panel) as well as longitudinal (lower panel) study designs are shown. IV, inverse variance.
Sensitivity analyses showed that the association of substantial occupational standing and low-back symptoms did not statistically differ when the threshold for substantial occupational standing was set at 2 hours/workday compared with 4 hours/workday (χ2=0.02, p=0.88; table 2, online supplementary appendix 10). Exposure–outcome associations unadjusted for confounders showed apparently stronger associations (1.32 (1.09 to 1.59)) than those adjusted for confounders (1.23 (1.02 to 1.47); table 2, online supplementary appendix 11). Exposure–outcome associations from studies on samples of workers in general appeared stronger (1.40 (1.20 to 1.62)) than from those on samples of specific occupational groups (1.24 (0.86 to 1.78); table 2, online supplementary appendix 12). Exposure–outcome association from studies with high methodological quality showed apparently stronger associations (1.38 (1.16 to 1.64)) than those from studies with low methodological quality (1.25 (0.85 to 1.82); table 2, online supplementary appendix 13). Regarding publication bias, visual inspection of the funnel plot (see online supplementary appendix 14) suggested some degree of asymmetry with some larger studies reporting lower ORs than smaller studies.
The remaining 23 studies (n=27 899 participants) that reported on the association between occupational standing and low-back symptoms could not be used in our meta-analysis as insufficient homogeneous evidence was provided. Nine studies reported on significant positive (ie, substantial standing being associated with the occurrence of low-back symptoms) associations,17 ,25 ,28 ,34 ,39 ,44 ,53 ,67 ,72 eight studies reported on comparable but non-significant associations,26 ,29 ,31 ,33 ,38 ,59 ,60 ,69 while in another six studies associations of occupational standing and low-back symptoms were assessed, but the outcomes of these associations were not reported (nor provided by the authors on request).27 ,30 ,35 ,47 ,58 ,61 These studies varied substantially in their definitions for exposure, outcome and exposure–outcome associations. Regarding variation in definitions of exposure, for example, one study showed that there was a significantly higher prevalence of low-back symptoms for workers who reported that their ‘work was hampered by standing’ compared with workers who reported that their ‘work was hampered by sitting’ (OR with 95% CI 3.07 (1.88 to 5.01)).35 In comparison, Hill et al38 showed that the prevalence of low-back symptoms was higher by every hour of occupational standing, though CIs were wide (OR with 95% CI 2.96 (0.73 to 12.10)). Substantial heterogeneity existed in the definitions of low-back symptoms (eg, with studies reporting on pain, discomfort and symptoms, acute and chronic and even low-back symptoms exacerbated by occupational standing).28 ,29 Finally, some studies reported on exposure–outcome associations using metrics other than ORs, such as correlations,44 prevalence rates33 ,60 and HRs.17
Lower extremity symptoms
A total of 14 articles (n=31 924 participants) reported on the association between occupational standing and lower extremity symptoms. Three articles were on lower extremity symptoms in general,33 ,35 ,47 one on hip/knee/feet symptoms combined,17 two on hip symptoms,56 ,69 six on knee symptoms,41 ,50 ,52 ,54 ,61 ,69 two on feet symptoms,51 ,52 two on upper leg symptoms32 ,52 and three on lower leg symptoms.32 ,39 ,52
Eight studies reported that substantial occupational standing was significantly associated with a higher prevalence of lower extremity symptoms (with point estimate ORs ranging from 1.23 to 3.95).17 ,32 ,35 ,39 ,47 ,50–52 Four studies reported comparable but non-statistically significant exposure–outcome associations (with point estimate ORs ranging from 1.10 to 1.70).33 ,41 ,56 ,69 One study found that substantial occupational standing was associated with a significantly lower prevalence of lower extremity symptoms.69 There were an additional four studies in which the association of occupational standing and lower extremity symptoms was assessed, but the outcomes of these associations were not reported.17 ,51 ,54 ,61
Upper extremity symptoms
A total of 18 articles (n=25 708 participants) reported on the association of occupational standing and upper extremity symptoms, of which 3 articles focused on upper extremity symptoms in general,33 ,35 ,47 5 on neck/shoulder symptoms,17 ,31 ,36 ,60 ,72 10 on neck symptoms,26 ,32 ,38 ,39 ,44 ,47 ,50 ,61 ,67 ,69 7 on shoulder symptoms,26 ,32 ,38 ,39 ,54 ,61 ,67 7 on forearm/hand and/or finger symptoms,17 ,26 ,32 ,38 ,54 ,60 ,69 and 1 on arm-only symptoms.32
Four studies reported substantial occupational standing to be significantly associated with a higher prevalence of upper extremity symptoms,17 ,35 ,36 ,44 nine studies reported comparable but non-statistically significant exposure–outcome associations,26 ,32 ,33 ,38 ,50 ,60 ,61 ,67 ,72 while one study found that substantial occupational standing was associated with a lower prevalence of upper extremity symptoms.32 There were another 10 studies in which the association of occupational standing and upper extremity symptoms was assessed, but the outcomes of these associations were not reported.17 ,31 ,32 ,35 ,39 ,47 ,50 ,54 ,61 ,69
Symptoms in any body area
Eight articles (n=3114 participants) reported on the association of occupational standing with musculoskeletal symptoms in any body area.17 ,24 ,40 ,45 ,46 ,50 ,55 ,57 Three studies reported that substantial occupational standing was significantly associated with a higher prevalence of symptoms. For example, significant associations for substantial standing with symptoms were found for standing more compared with <30 min/hour ((HR with 95% CI) 1.6 (1.2 to 2.3)),17 and for standing more or <4 hours/workday ((OR with 95% CI) 3.67 (1.88 to 7.17)).55 One study reported substantial occupational standing to be associated with a reduced prevalence of symptoms compared with rarely standing (OR 0.56 (0.34 to 0.94)).40 Two studies reported on non-significant associations of occupational standing and symptoms in any body area.45 ,57 Two studies in which the association of occupational standing and lower extremity symptoms was assessed reported no outcomes of these associations.46 ,50
Discussion
Meta-analysis evidence from 16 articles with 54 392 participants suggested a statistically significant association between substantial occupational standing and the occurrence of low-back symptoms with a pooled OR (with 95% CI) of 1.31 (1.10 to 1.56). The association remained whether the cut-off value for substantial occupational standing was 2 or 4 hours/workday; however, due to insufficient data, we could not explore other cut-off values (eg, 6 hours/workday). Therefore, at present, we cannot draw conclusions on the dose–response association of substantial standing and low-back symptoms (ie, how much standing should be considered excessive). Also evidence from studies not analysed in the meta-analysis (23 articles with n=27 899 participants) indicated an association of substantial occupational standing with the occurrence of low-back symptoms.
Our findings are broadly in line with what has been reported in a (non-systematic) review previously,12 but contrast with the conclusions of several other reviews.16 ,18 ,19 One reason for the contrasting conclusions is the addition of a considerable body of recent evidence in the current review (17 out of the 50 included articles being published since 2010). A further reason for the contrasting conclusions is that some prior reviews attempted to prove a causal relationship, whereas this review assessed the epidemiological evidence for an association. Experimental laboratory studies have consistently demonstrated musculoskeletal symptoms in the low-back and lower limbs increase over several hours of standing,73 ,74 suggesting a causal relationship may exist with occupational exposure and symptoms. However, the strength of epidemiological evidence is not in demonstrating causal relationships, and the reviews which made strong conclusions about the (lack of) causal relationships based on available epidemiological studies have been strongly criticised.20 ,21 What is clear from all available reviews is that further evidence—from high-quality, longitudinal epidemiological studies using objective measures of occupational standing and from laboratory studies—is needed to provide more convincing evidence of an association. Such studies can also help to determine the dose-response relationship, understand the mechanisms (eg, muscle fatigue75 and postural changes76 ,77) and provide evidence for thresholds of excessive standing.
Although we were not able to perform a meta-analysis for the association of occupational standing and lower limb symptoms, the available evidence suggests (although inconclusively) an association between substantial occupational standing and the occurrence of lower extremity symptoms. These findings are in line with what has been reported before for some epidemiological70 and laboratory studies.73 ,78 Similar to the associations for occupational standing with low-back symptoms, future epidemiological and laboratory research may help to explain the association between substantial occupational standing and lower extremity symptoms, may provide evidence for thresholds of excessive standing and should be explored to understand the mechanisms (eg, muscle fatigue79 and other non-musculoskeletal vascular mechanisms such as swelling,80 due to blood pooling in the lower limbs75). Evidence to date does not indicate a significant association of occupational standing and upper limb symptoms (either positive or negative).
Methodological considerations
Considerable evidence on the association of occupational standing with musculoskeletal symptoms was found (with data from n=88 158 participants). However, due to the large heterogeneity between studies, data were difficult to synthesise. Sources of heterogeneity included differences in the definitions of the exposure (ie, occupational standing) and outcome (ie, musculoskeletal symptoms); differences in study designs and study samples; and the methodological quality of the identified studies.
The majority of the articles described studies that were based on cross-sectional designs, and thus inferences with regard to causality—including the direction of the associations—cannot be determined. While the occurrence of musculoskeletal symptoms as a result of exposure to occupational standing is discussed in most of the identified evidence (taking a traditional ergonomics perspective), it could also be possible that participants with symptoms adopt different activity behaviours than participants without symptoms,81 with variation in posture often seen as a strategy for relief from pain.82 In the subset of studies that used a longitudinal design, a weaker and not statistically significant association was found, reinforcing the need for caution in interpreting the cross-sectional findings.
The vast majority of the studies assessed occupational standing by self-report measures. As such, some moving may also have been captured by these measures, which may have influenced the association with musculoskeletal symptoms. Objective measures of occupational exposure are preferred,83 and are better able to detect true exposure–outcome associations.84 Moreover, objective measures (eg, using posture based monitors) allow for a more detailed assessment of activities (such as standing) that include not just the total amount of activities, but also patterns of activities. For example, a single 4-hour period of static standing is likely to have different musculoskeletal consequences than 4 hours of standing accrued in short (eg, <20 min) bouts throughout the workday. There was also substantial variation in the operationalisation of occupational standing (eg, standing in hours/day, hours/week, minutes/hour or even years of exposure). Similarly, the variation in the definitions of musculoskeletal symptoms was substantial, with variation in period (eg, symptoms in the past 7 days, last month or last year), operationalisation of the symptoms (eg, defining the intensity of symptoms or the yes/no presence of symptoms) and body area of symptoms. Harmonising certain definitions would enhance synthesis of the evidence.
We found stronger associations in studies with high methodological quality compared with those with low methodological quality, supporting the value of high-quality studies. It should be noted though that the methodological quality scale did not distinguish cross-sectional from longitudinal studies. One of the issues around methodological quality was the adjustment for confounders (or not). Heterogeneity in adjustments for confounding (ie, in the variables—if any—used) was too great to allow meta-analysis on associations adjusted for confounders. However, sensitivity analysis showed weaker associations among evidence from studies that adjusted for confounders. This suggests the importance of considering confounding or mediating variables (including gender, age, other physical or mental work demands, and previous musculoskeletal symptoms) that could explain or modify the association of occupational standing with musculoskeletal symptoms. These findings suggest that the current results (that are mainly based on unadjusted associations) should be interpreted with care, and that influencing variables should be considered in future research.
Studies with samples that included various occupations (ie, a combination of various occupations or random samples of a general working population) had stronger exposure–outcome associations than those that were reported from specific occupational groups (eg, healthcare, factory or construction workers), although no significant subgroup differences were observed. These specific occupational groups are likely to have a similar occupational exposure (ie, either standing a lot or sitting a lot) and a lack of within-group variation in occupational standing and symptoms may explain the weaker exposure–outcome associations found.85 The ‘healthy-worker-effect’, in which workers without symptoms are more likely to remain in physically demanding jobs,86 may also play a role in these findings.
With some level of asymmetry in the funnel plot from studies that were included in the meta-analysis and a number of studies not reporting on (potentially non-significant) associations, publication bias might be present. Current results should therefore be interpreted with caution. Furthermore, a limitation of the current review is that it was not registered a priori.
Conclusion
This systematic review found evidence for associations between substantial occupational standing and the occurrence of low-back symptoms (pooled OR of 1.31 (1.10 to 1.56)) and (inconclusively) lower extremity symptoms. The evidence did not support a significant or meaningful association of occupational standing with upper extremity symptoms. However, these conclusions are tentative as there was only limited evidence from high-quality, longitudinal studies using objectively measured occupational standing, fully adjusted models and well-characterised symptom outcomes. More information is needed in order to provide more definitive evidence to inform good work design.
What is already known?
There are high exposures to occupational standing in specific occupations and recent initiatives encouraging intermittent standing among white-collar workers.
In light of these (shifting) working styles, some concerns have been expressed that occupational standing may expose workers to risks of health consequences such as musculoskeletal symptoms.
The association of occupational standing with musculoskeletal symptoms is currently unclear, with no current systematic review investigating this association.
What are the findings?
We systematically reviewed literature and identified substantial evidence (50 articles from n=88 158 participants) describing associations of occupational standing with low-back, lower extremity and upper extremity symptoms.
We found evidence (including pooled data from a meta-analysis) for associations between occupational standing and the occurrence of low-back and (inconclusively) lower extremity symptoms, however not for upper extremity symptoms.
Only limited evidence from high-quality, longitudinal studies (5 articles from n=10 633 participants) using objectively measured standing (2 articles from n=83 participants) was found.
Information on the association of occupational standing and musculoskeletal symptoms is needed to provide more definitive evidence to inform good work design for both blue-collar and white-collar workers.
Acknowledgments
GNH was supported by a NHMRC Career Development Fellowship (NHMRC #108029). DWD was supported by a NHMRC Senior Research Fellowship (NHMRC #1078360). LMS was supported by a NHMRC Senior Research Fellowship (NHMRC #1019980). CGM was supported by a NHMRC Principal Research Fellowship (NHMRC #1103022). The authors are grateful for the financial assistance from the Victorian Government's OIS Program.
References
Footnotes
Twitter Follow Pieter Coenen @coenen_pieter, Christopher Maher @CGMMaher, Genevieve Healy @genevieve_healy and Leon Straker @Leon_Straker
Contributors PC, LW, SP and JWS conducted literature screening and data extraction of all included papers. LR and DMB conducted the literature search in electronic data bases. All authors (PC, LW, SP, JWS, LR, DMB, CGM, GNH, DWD and LMS) analysed the data and reviewed the manuscript for important intellectual content. LMS is the guarantor.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.